
A Silent Epidemic You May Not Know About
Every year, millions of people visit their doctor for routine checkups and walk away with a clean bill of health, at least on the surface. Their cholesterol is borderline, their blood pressure is slightly elevated, they carry a little extra weight around the abdomen, and they feel more tired than they used to. Individually, each of these findings seems manageable, even unremarkable. But together, they may be telling a very different story.
Welcome to the world of Cardiovascular-Kidney-Metabolic (CKM) Syndrome, a closely interconnected cluster of health conditions that is now being called one of the most significant silent epidemics of the 21st century.
"CKM Syndrome is not one disease. It is the quiet convergence of many, each condition silently amplifying the others, often for years before the damage becomes visible." |
In 2023, the American Heart Association published a landmark scientific statement formally recognizing CKM Syndrome as a distinct, integrated health condition, one that links cardiovascular disease, kidney disease, obesity, and metabolic dysfunction in a way that demands a unified clinical and lifestyle response. Since then, clinicians, preventive medicine specialists, and public health researchers have been working to raise awareness of how widespread, and how underdiagnosed, this syndrome truly is.
The numbers are sobering. Estimates suggest that more than one-third of adults in developed countries may currently exist at one of the early stages of CKM syndrome, many without knowing it. The interconnected nature of the condition means that allowing one component, say, unmanaged blood pressure or creeping weight gain, to go unaddressed can accelerate damage across multiple organ systems simultaneously.
The good news? CKM Syndrome is not a death sentence. It is a wake-up call. Early detection, evidence-based lifestyle changes, and consistent cardiometabolic monitoring can slow, halt, or even partially reverse the progression of CKM Syndrome for many people. This article is designed to give you exactly what you need: understanding, clarity, and a practical, compassionate roadmap for prevention in 2026.

SECTION 2
What Is CKM Syndrome?
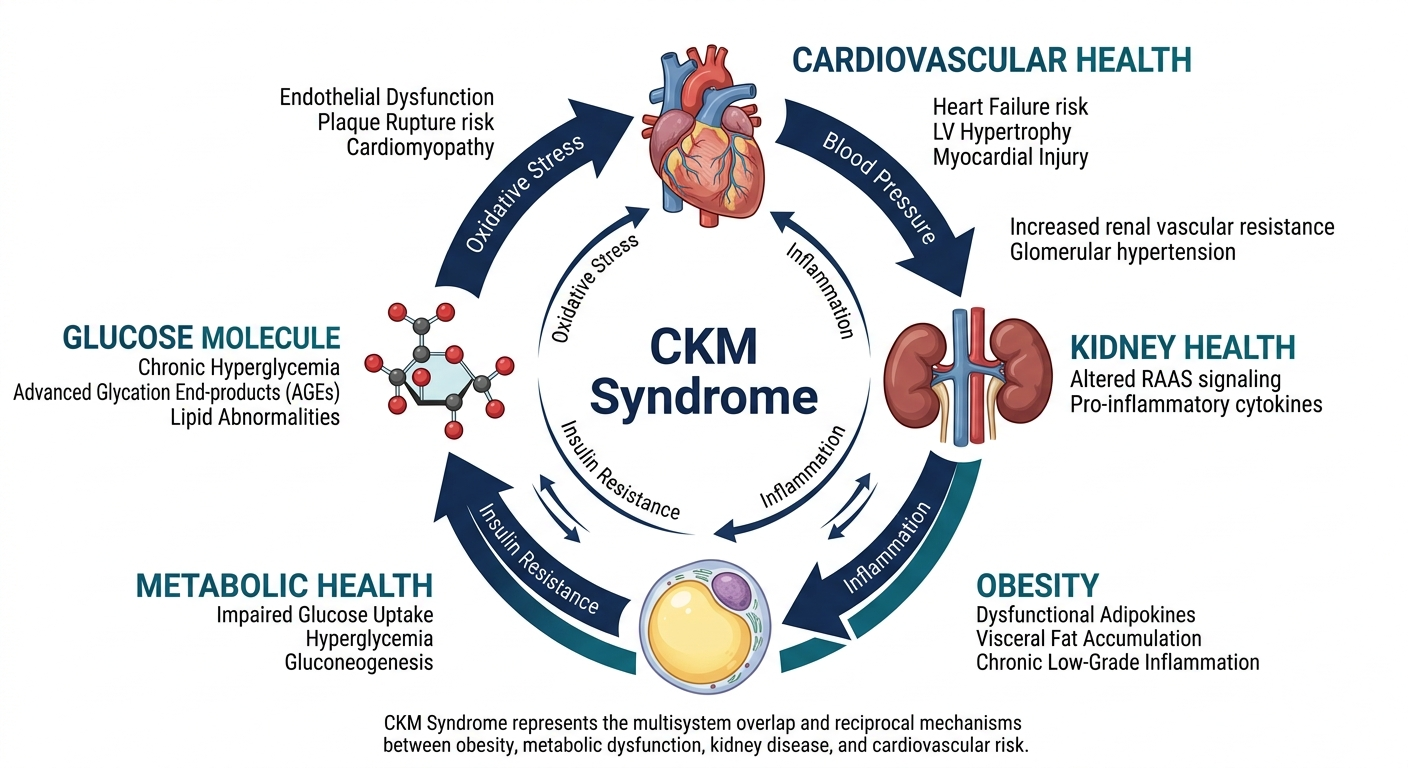
Cardiovascular-Kidney-Metabolic (CKM) Syndrome is a term used to describe the complex, bidirectional interaction between three interconnected domains of health: cardiovascular disease, chronic kidney disease (CKD), and metabolic dysfunction, which encompasses conditions like obesity, type 2 diabetes, insulin resistance, and dyslipidemia.
The defining feature of CKM Syndrome is not just the presence of these individual conditions, but the way they reinforce and accelerate one another. The heart, the kidneys, and the metabolic system are biologically intertwined through shared mechanisms, inflammation, insulin signaling, blood pressure regulation, fluid balance, and endothelial (blood vessel lining) health. When one system falters, the others are dragged down with it.
The Four Pillars of CKM Syndrome
Condition | How It Connects to CKM Syndrome |
|---|---|
Cardiovascular Disease | High blood pressure, arterial inflammation, and atherosclerosis damage kidney filtration and worsen metabolic dysfunction. Poor heart output reduces oxygen and nutrients to organ systems. |
Chronic Kidney Disease (CKD) | Declining kidney function leads to fluid and toxin accumulation, blood pressure dysregulation, and anemia — all of which place increased strain on the heart and disrupt metabolic balance. |
Obesity / Excess Adiposity | Visceral fat (fat around internal organs) drives systemic inflammation, insulin resistance, hormonal disruption, and direct mechanical pressure on kidneys and the cardiovascular system. |
Metabolic Dysfunction (Diabetes / Prediabetes / Insulin Resistance) | Chronically elevated blood glucose damages blood vessels and kidney filters (nephrons), accelerating both cardiovascular and renal decline. Insulin resistance dysregulates nearly every organ system involved. |
The CKM Staging Framework
The American Heart Association's 2023 framework describes CKM Syndrome across five stages, from Stage 0 (no CKM risk factors) through Stage 4 (established cardiovascular disease with kidney disease and metabolic dysfunction). Most adults who are at risk currently sit in Stages 1 through 3, often unaware of their trajectory.
Stage 0:
No CKM risk factors. Healthy metabolic profile, normal kidney function, no cardiovascular disease.
Stage 1:
Excess weight, abdominal obesity, or borderline blood sugar — without kidney disease or cardiovascular events.
Stage 2:
Metabolic risk factors plus kidney disease, hypertension, or elevated cardiovascular risk scores.
Stage 3:
Subclinical cardiovascular disease present (detectable by imaging or biomarkers) alongside metabolic and kidney findings.
Stage 4:
Established cardiovascular events (heart attack, stroke, heart failure) in the context of CKM syndrome.
SECTION 3
Why CKM Syndrome Is Rising Rapidly in 2026
CKM Syndrome does not arise from a single cause. It is the product of decades of shifting lifestyle patterns, environmental pressures, and biological vulnerabilities that have reached a critical intersection in the modern world. Understanding why CKM Syndrome is on the rise is not about assigning blame, it is about identifying the levers we can pull to change course.
The Driving Forces Behind the CKM Epidemic
Risk Factor | How It Contributes to CKM Syndrome |
|---|---|
| Sedentary Lifestyle | Physical inactivity reduces insulin sensitivity, raises blood pressure, promotes visceral fat accumulation, and accelerates cardiometabolic decline. The global shift toward desk-based and screen-based work has made sedentary behavior the default for hundreds of millions. |
| Ultra-Processed Diet | Diets high in refined carbohydrates, added sugars, trans fats, and sodium drive insulin resistance, systemic inflammation, hypertension, dyslipidemia, and renal strain — all key drivers of CKM progression. |
| Chronic Stress | Prolonged stress elevates cortisol and adrenaline, driving blood pressure, blood sugar, and visceral fat storage. Chronic psychological stress is now recognized as an independent risk factor for cardiometabolic disease. |
| Poor Sleep Quality | Short or disrupted sleep impairs glucose metabolism, raises inflammatory markers, disrupts appetite-regulating hormones (leptin and ghrelin), and elevates blood pressure. Adults sleeping fewer than 6 hours are at measurably higher cardiometabolic risk. |
| Global Obesity Epidemic | More than 1 billion adults worldwide now live with obesity. Excess visceral adiposity is the central driver of insulin resistance, inflammation, and the downstream organ damage that defines CKM syndrome. |
| Insulin Resistance | Increasingly common due to dietary patterns and physical inactivity, insulin resistance sits at the metabolic core of CKM syndrome — disrupting glucose handling, promoting vascular damage, and accelerating kidney filtration loss. |
| Aging Populations | CKM risk compounds with age. As the global population ages, the prevalence of overlapping metabolic, cardiovascular, and renal risk factors naturally increases. |
| Digital Lifestyle Habits | Increased screen time, disrupted circadian rhythms from blue light exposure, social media stress, and digital-era convenience food ordering have all been identified as contributors to sedentary, metabolically disruptive lifestyles. |
"We are living in a metabolic environment that our biology was never designed to navigate. The result is a slow, systemic overload, invisible at first, but cumulative and consequential."
SECTION 4
Early Warning Signs Most People Ignore
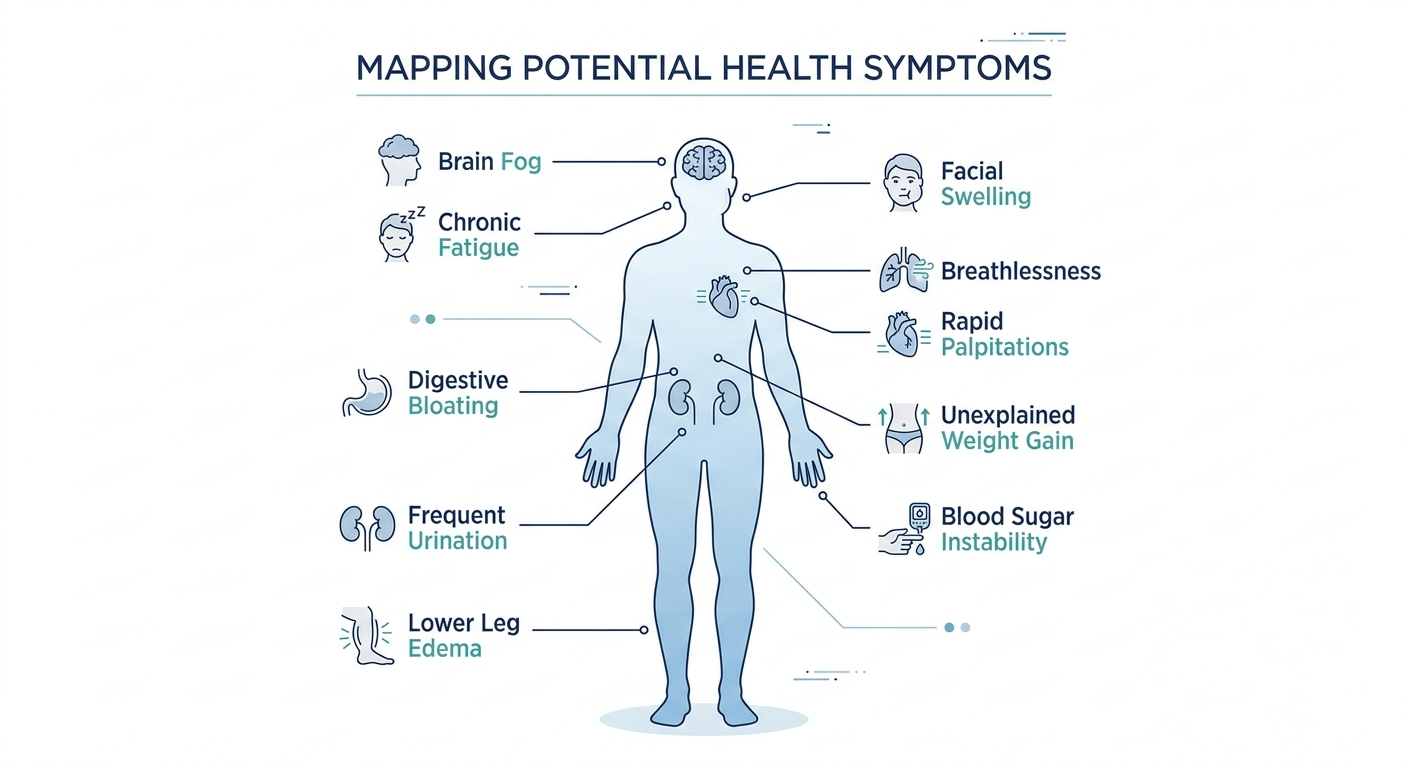
One of the most dangerous characteristics of early-stage CKM Syndrome is how ordinary its symptoms feel. The signals are often vague, gradual, and easily attributed to aging, stress, or a busy lifestyle. But for those who know what to look for, these early clues are invaluable opportunities to intervene before serious damage occurs.
The 10 Warning Signs Worth Taking Seriously
Persistent, unexplained fatigue
Particularly fatigue that worsens after meals or does not improve with adequate sleep — can reflect insulin resistance, anemia of kidney disease, or reduced cardiac output.
Elevated blood pressure
Even readings in the 'high-normal' range (130–139/80–89 mmHg) — are now recognized as clinically significant and are associated with accelerated kidney damage and cardiovascular risk.
Gradual, unexplained weight gain
Particularly around the abdomen — indicates rising visceral adiposity, which directly drives insulin resistance, inflammation, and hormonal dysfunction.
Brain fog and difficulty concentrating
Cognitive cloudiness is associated with insulin resistance, elevated blood glucose, poor sleep quality, and early-stage kidney dysfunction affecting toxin clearance.
Ankle, leg, or facial swelling (edema)
Fluid retention can reflect declining kidney function, heart strain, or hypoalbuminemia (low blood protein) related to kidney disease.
Frequent urination, especially at night
Nocturia and increased urinary frequency can signal early kidney dysfunction, poorly controlled blood sugar, or developing hypertension.
Poor or non-restorative sleep
Difficulty falling asleep, staying asleep, or waking unrefreshed is both a cause and a consequence of metabolic dysfunction.
Blood sugar instability
Energy crashes after meals, cravings for sugar and refined carbs, and irregular appetite may indicate insulin resistance or prediabetes.
Shortness of breath on mild exertion
A subtle reduction in cardiovascular fitness or early cardiac changes can manifest as mild breathlessness during activities that previously felt easy.
Elevated cholesterol or triglycerides on routine bloodwork
Dyslipidemia, particularly high triglycerides combined with low HDL cholesterol, is a hallmark metabolic warning sign of CKM risk.
IMPORTANT: The Cumulative Effect |
|---|
No single symptom on this list is diagnostic of CKM Syndrome on its own. |
It is the PATTERN of multiple overlapping signals, combined with laboratory findings and risk factors, that defines CKM risk. |
If you recognize three or more of these patterns in yourself, discuss a comprehensive cardiometabolic screening with your healthcare provider. |
Early detection dramatically changes outcomes. |
SECTION 5
Who Is Most at Risk?
While CKM Syndrome can affect virtually any adult, certain profiles carry substantially higher risk. Identifying your personal risk landscape is the first step toward targeted, effective prevention.
High-Risk Profiles
Risk Profile | Why the Risk Is Elevated |
|---|---|
| Adults aged 35 and older | Metabolic rate naturally slows, insulin sensitivity declines, cardiovascular stiffness increases, and cumulative lifestyle exposures compound over decades. |
| Individuals living with obesity | Visceral adiposity is the central metabolic driver of CKM Syndrome, fueling inflammation, insulin resistance, and direct organ stress across all three domains. |
| People with type 2 diabetes or prediabetes | Chronic hyperglycemia damages blood vessels and kidney nephrons directly, dramatically accelerating cardiovascular and renal disease progression. |
| Hypertensive individuals | High blood pressure is simultaneously a cause and consequence of CKM Syndrome, driving renal damage and cardiac remodeling across organ systems. |
| Smokers and tobacco users | Smoking accelerates endothelial dysfunction, promotes inflammation, reduces kidney perfusion, and independently raises cardiovascular and metabolic risk. |
| Sedentary individuals | Lack of regular physical activity drives insulin resistance, visceral fat accumulation, elevated blood pressure, and impaired cardiovascular fitness. |
| People with family history of heart disease, diabetes, or CKD | Genetic predispositions significantly amplify environmental and lifestyle risks, making early screening especially important. |
| Chronically stressed individuals | High cortisol environments promote visceral fat, blood pressure elevation, blood sugar instability, and immune dysregulation. |
| Individuals with poor dietary habits | High-sodium, high-sugar, low-fiber, ultra-processed food patterns accelerate every component of CKM Syndrome. |
| People of South Asian, African, or Hispanic descent | Certain ethnic groups carry higher genetic susceptibility to insulin resistance, visceral adiposity, and cardiometabolic disease, often at lower BMI thresholds than traditional reference ranges suggest. |
"Risk is not destiny. But understanding your risk is the single most empowering thing you can do for your long-term health. Awareness is the foundation of prevention."
SECTION 6
How CKM Syndrome Affects the Body
To truly understand CKM Syndrome, it helps to understand the underlying biological mechanisms — the internal processes by which these interconnected conditions damage the body over time. This is not about alarm; it is about biological literacy. Understanding what is happening inside creates the motivation to change what is happening outside.
Key Biological Mechanisms
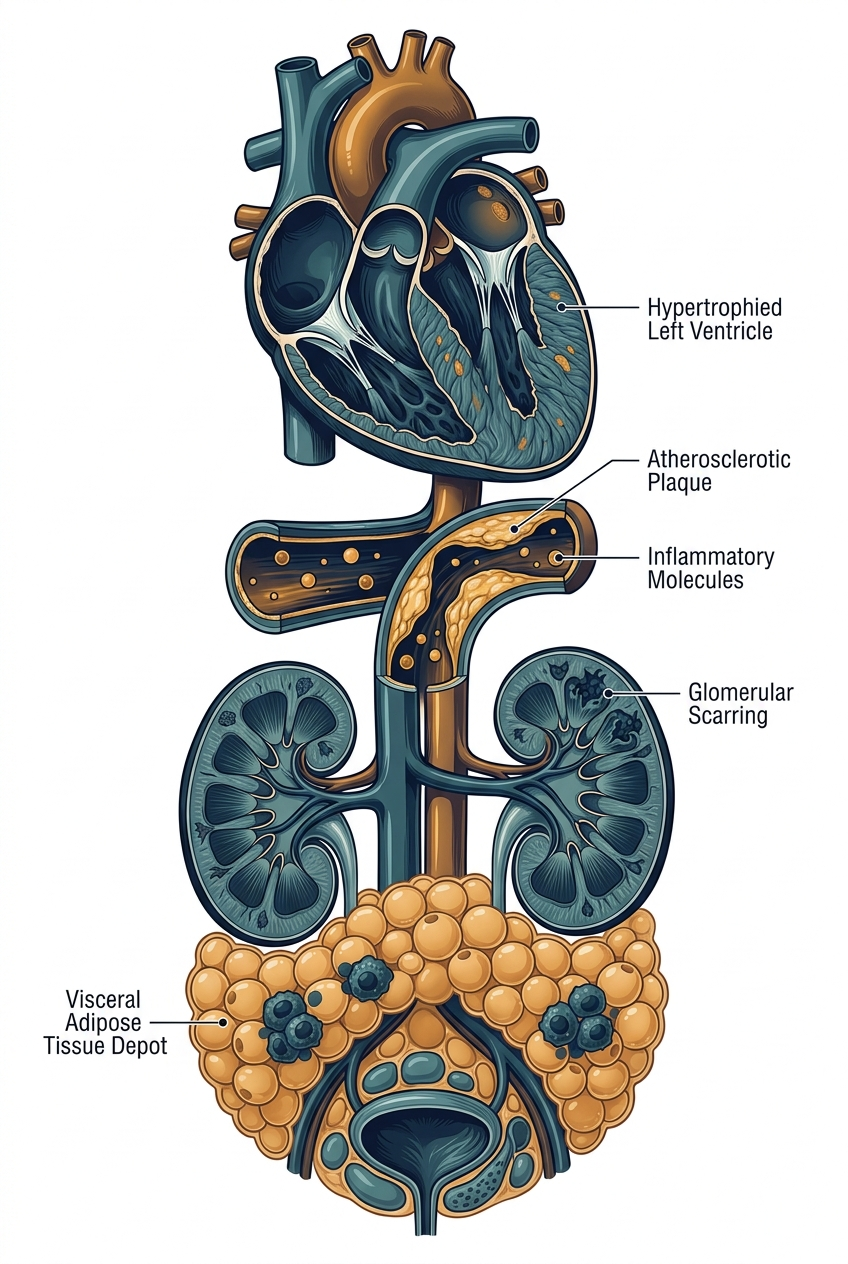
1. Chronic Low-Grade Inflammation
Visceral fat — the fat that accumulates around the internal organs, is not simply inert storage tissue. It is biologically active, producing pro-inflammatory cytokines (chemical messengers) such as TNF-alpha, IL-6, and CRP. This creates a state of chronic, low-grade systemic inflammation that silently damages blood vessels, disrupts insulin signaling, strains the kidneys, and accelerates atherosclerosis (plaque buildup in arteries).
2. Insulin Resistance and Blood Glucose Dysregulation
Insulin resistance occurs when the body's cells stop responding efficiently to insulin, the hormone that enables glucose to enter cells for energy. As resistance deepens, the pancreas compensates by producing more insulin, leading to chronically elevated insulin levels (hyperinsulinemia). Over time, blood glucose rises, damaging the tiny blood vessels (capillaries) in the kidneys, heart, eyes, and nerves. This vascular damage is one of the core mechanisms linking diabetes to both kidney disease and cardiovascular disease in CKM Syndrome.
3. Endothelial Dysfunction
The endothelium is the thin inner lining of all blood vessels. In CKM Syndrome, chronic inflammation, oxidative stress, and elevated blood glucose impair the endothelium's ability to regulate blood flow, prevent clotting, and maintain vascular tone. Endothelial dysfunction is an early, measurable precursor to atherosclerosis and represents a critical window for prevention.
4. Kidney Filtration Decline
The kidneys contain approximately one million filtration units each (nephrons), which constantly filter blood and regulate fluid, electrolyte, and waste balance. In CKM Syndrome, high blood pressure mechanically stresses nephrons; diabetic nephropathy (kidney damage from high blood sugar) scars renal tissue; and inflammatory mediators further reduce filtration efficiency. As the glomerular filtration rate (GFR) declines, the kidneys lose their ability to regulate blood pressure, clear metabolic waste, and produce hormones that support red blood cell production, creating a vicious cycle with cardiovascular and metabolic systems.
5. Cardiac Structural and Functional Changes
Chronically elevated blood pressure forces the heart to pump against greater resistance, leading to left ventricular hypertrophy (thickening of the heart's main pumping chamber). Simultaneously, atherosclerosis reduces coronary artery blood flow, and metabolic dysfunction reduces the heart's energy efficiency. Over time, these changes manifest as reduced exercise tolerance, heart failure, arrhythmias, and ultimately, major cardiovascular events.
Please note: this is for informational purposes only. For medical advice or diagnosis, consult a professional.
SECTION 7
The 2026 Daily Prevention & Recovery Protocol
Prevention is not a single dramatic intervention. It is the accumulation of daily choices, small, consistent behaviors that compound over weeks, months, and years into dramatically different health outcomes. The following protocol integrates current clinical guidelines with practical, sustainable lifestyle medicine principles.
"The most powerful medicine for CKM Syndrome is not in a bottle, it is in your daily routine. Sleep, movement, nutrition, and stress management are the four pillars of metabolic restoration."
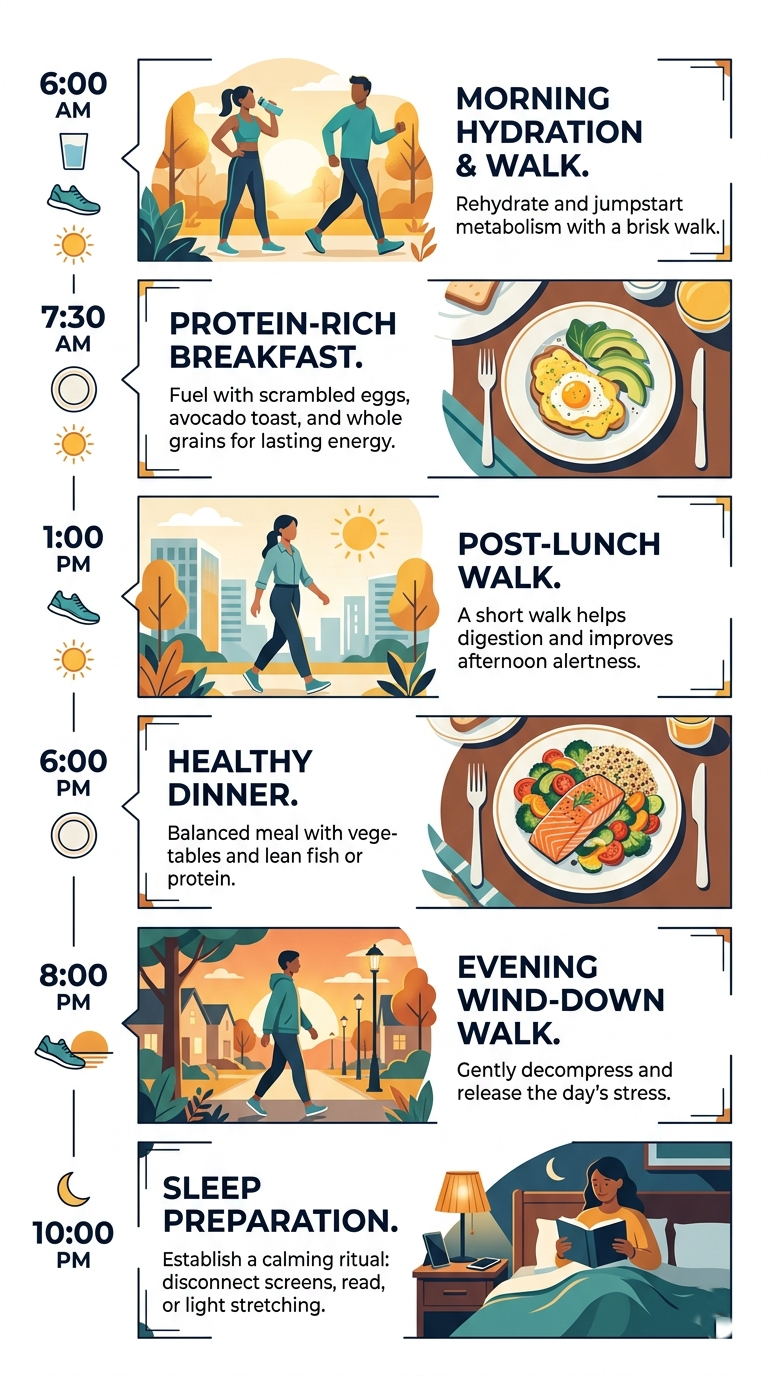
Morning Protocol (6:00–9:00 AM)
Begin with hydration:
16 oz of water before any food or beverage. The kidneys cleared metabolic waste overnight and need fluid to reset.
Move before the day takes over:
A 20–30 minute morning walk, gentle yoga, or resistance training session dramatically improves insulin sensitivity for hours afterward.
Breakfast priorities:
High-fiber, protein-rich, low-glycemic. Prioritize whole eggs, Greek yogurt, or plant-based protein with vegetables. Avoid refined cereals, fruit juices, and high-sugar coffee beverages.
Morning monitoring:
If using a continuous glucose monitor (CGM) or a blood pressure cuff, take your readings before eating. Track patterns, not individual data points.
Mindful start:
5–10 minutes of intentional breathing, meditation, or quiet reflection before screen exposure has measurable cortisol-lowering effects.
Midday Protocol (12:00–2:00 PM)
Lunch composition:
Half the plate with non-starchy vegetables, a quarter with lean protein (fish, legumes, chicken), and a quarter with whole grain or starchy vegetable. Keep sodium moderate.
Post-meal movement:
Even a 10-minute walk after lunch blunts the blood glucose spike from food, a simple, highly effective cardiometabolic intervention.
Hydration check:
Urine should be pale yellow. If darker, increase water intake. Kidney health is directly tied to adequate daily hydration.
Avoid the afternoon sedentary collapse:
If desk-bound, stand, stretch, or walk for 2–5 minutes every 45–60 minutes. Prolonged unbroken sitting is independently associated with cardiometabolic risk.
Stress checkpoint:
Brief mid-day decompression, stepping outside, deep breathing, or a short walk, interrupts the cortisol accumulation that drives visceral fat storage.
Evening Protocol (5:00–10:00 PM)
Dinner timing:
Aim to finish eating 2–3 hours before bedtime to optimize glucose metabolism and sleep quality.
Dinner composition:
Similar principles to lunch. Emphasize fish (especially oily fish twice weekly), legumes, leafy greens, and whole grains. Minimize alcohol, which disrupts both sleep architecture and blood sugar regulation.
Evening movement:
A gentle evening walk (15–20 minutes) after dinner is one of the most consistently evidence-supported strategies for blood sugar and blood pressure management.
Screen hygiene:
Reduce blue-light exposure in the hour before bed. Blue light suppresses melatonin, disrupts circadian rhythm, and — through sleep disruption — elevates next-morning cortisol and insulin resistance.
Sleep preparation:
Target 7–9 hours. Consistent sleep and wake times reinforce the circadian rhythm that regulates metabolic hormones, blood pressure, and inflammatory responses.
Weekly CKM Health Habits Checklist
| CKM Prevention Weekly Checklist |
| [ ] 150+ minutes of moderate aerobic exercise completed (30 min x 5 days) |
| [ ] 2+ resistance/strength training sessions |
| [ ] 7 servings of vegetables and fruits (prioritize non-starchy) |
| [ ] 2 servings of oily fish (salmon, mackerel, sardines) OR omega-3 supplement taken |
| [ ] Alcohol kept within low-risk guidelines (or eliminated) |
| [ ] Average 7–9 hours of sleep per night achieved |
| [ ] Blood pressure measured and recorded |
| [ ] Blood sugar monitored (if prediabetic or diabetic) |
| [ ] Hydration maintained (8+ cups of water daily) |
| [ ] Stress management practice completed (mindfulness, breathing, nature walk) |
| [ ] No more than 2 ultra-processed meals this week |
| [ ] Healthcare appointment scheduled or completed (for those in Stages 2–4) |
SECTION 8
Best Foods for CKM Syndrome Prevention
Food is not merely fuel, for individuals with CKM risk, it is medicine. The nutritional choices you make three times a day have measurable, compounding effects on blood pressure, blood sugar, kidney function, cardiovascular inflammation, and metabolic efficiency. The following evidence-based dietary guidance draws from Mediterranean dietary principles, DASH (Dietary Approaches to Stop Hypertension) protocols, and current clinical nutrition recommendations for cardiometabolic and renal health.
Top Foods to Prioritize
Food Category | CKM Benefits |
|---|---|
Oily Fish (salmon, mackerel, sardines, herring) | Rich in omega-3 fatty acids (EPA and DHA), which reduce triglycerides, lower systemic inflammation, support endothelial function, and have modest blood pressure-lowering effects. |
Leafy Green Vegetables (spinach, kale, arugula, Swiss chard) | High in nitrates (supporting blood pressure regulation), magnesium, potassium, fiber, and antioxidants. Consistently associated with reduced cardiovascular and metabolic risk in large population studies. |
Legumes (lentils, chickpeas, black beans, kidney beans) | Exceptional sources of soluble fiber, plant protein, and resistant starch — all of which improve insulin sensitivity, reduce LDL cholesterol, and support microbiome health. Also kidney-friendly when consumed appropriately. |
Whole Grains (oats, quinoa, barley, brown rice, farro) | Soluble beta-glucan fiber in oats lowers LDL cholesterol; whole grains reduce glycemic response compared to refined counterparts and are associated with lower cardiometabolic risk. |
Berries (blueberries, strawberries, raspberries) | Among the highest antioxidant foods available. Anthocyanins in berries have been linked to reduced blood pressure, improved endothelial function, and lower systemic inflammation. |
Extra Virgin Olive Oil | The cornerstone fat of the Mediterranean diet. Rich in oleocanthal (anti-inflammatory) and oleic acid. Associated with reduced cardiovascular events, improved insulin sensitivity, and anti-inflammatory effects. |
Nuts and Seeds (walnuts, almonds, flaxseed, chia seeds) | Heart-healthy fats, fiber, plant sterols, and magnesium. Walnuts in particular provide plant-based omega-3s and are consistently associated with improved cardiometabolic markers. |
Garlic and Onions | Both contain compounds (allicin in garlic; quercetin in onions) with documented blood pressure-lowering, anti-inflammatory, and cardioprotective properties. |
Green Tea and Herbal Teas | Polyphenols in green tea (particularly EGCG) have been associated with improved insulin sensitivity, modest blood pressure reduction, and reduced inflammatory markers. |
Fermented Foods (plain yogurt, kefir, kimchi, sauerkraut) | Support a diverse gut microbiome, which plays an increasingly recognized role in metabolic health, inflammation regulation, and cardiometabolic risk modulation. |
Foods to Reduce or Avoid
Food / Category | Why It Increases CKM Risk |
|---|---|
| Ultra-processed foods (packaged snacks, fast food, processed meats) | High in sodium, added sugars, refined carbohydrates, industrial seed oils, and additives — driving inflammation, insulin resistance, blood pressure elevation, and renal stress. |
| Sugar-sweetened beverages (sodas, energy drinks, fruit juices) | Provide rapidly absorbed fructose and glucose with no fiber buffer — spiking blood sugar, raising triglycerides, and driving hepatic (liver) fat accumulation and insulin resistance. |
| Excess sodium (high-salt processed foods, table salt overuse) | Directly raises blood pressure and increases glomerular hyperfiltration — one of the earliest forms of kidney damage in at-risk individuals. |
| Refined carbohydrates (white bread, white rice, pastries, crackers) | Rapidly digested carbohydrates spike blood glucose and insulin, contributing to insulin resistance and metabolic dysfunction over time. |
| Alcohol | Regular alcohol consumption raises blood pressure, disrupts sleep, elevates triglycerides, strains the liver, and contributes to visceral fat accumulation. |
| Red and processed meats (in excess) | Associated with elevated cardiovascular risk and, in individuals with kidney disease, requires careful moderation due to protein and phosphorus load. |
"Eating a Mediterranean-style diet, abundant in plants, whole grains, fish, and healthy fats, while limiting processed foods and added sugars, remains the single most evidence-backed dietary pattern for CKM prevention." |

SECTION 9
Supplements Commonly Discussed for CKM Support
Before discussing specific supplements, it is important to state clearly: no supplement can replace the foundational lifestyle interventions of nutrition, exercise, sleep, and stress management. Supplements may play a supporting role for some individuals, but the evidence base varies considerably between compounds, and safety considerations (particularly for those with kidney disease) mean that any supplementation should be discussed with a qualified healthcare provider.
Key Supplements: Evidence Overview
Supplement | Potential Benefits | Evidence Level | Safety Notes |
|---|---|---|---|
| Omega-3 Fatty Acids (Fish Oil) | Reduces triglycerides, lowers inflammation, supports endothelial function, modest blood pressure effect | Strong — multiple RCTs and meta-analyses | Generally safe; high doses may affect platelet function. Discuss with doctor if on blood thinners. |
| Berberine | Improves insulin sensitivity, lowers blood glucose, modest LDL-lowering effects — mechanisms overlap with metformin | Moderate — promising but fewer large RCTs than pharmaceutical comparators | May interact with diabetes medications. Not recommended in kidney disease without medical guidance. |
| Magnesium (glycinate or malate) | Supports blood pressure regulation, insulin receptor function, sleep quality, and muscle relaxation | Moderate — especially for those with dietary deficiency, which is common | Avoid magnesium oxide (poor absorption). Use caution in kidney disease — reduced magnesium excretion. |
| Coenzyme Q10 (CoQ10) | Supports mitochondrial energy production, antioxidant properties, modest blood pressure effects | Moderate for blood pressure; limited evidence for other CKM outcomes | Well tolerated. May be particularly relevant for those on statin medications, which deplete CoQ10. |
| Vitamin D | Immune regulation, insulin sensitivity, cardiovascular function; deficiency highly prevalent and associated with worse CKM outcomes | Moderate — deficiency correction is supported; megadosing is not | Testing vitamin D levels before supplementing is recommended. Excessive vitamin D is toxic. |
| Psyllium Husk (Fiber Supplement) | Reduces LDL cholesterol, blunts postprandial glucose spikes, supports gut microbiome and renal health through reduced uremic toxin generation | Strong for lipids; moderate for glucose; growing evidence for renal benefits | Take with adequate water. May slow absorption of medications, take separately. |
IMPORTANT DISCLAIMER
This section is for informational and educational purposes only and does not constitute medical advice.
Individuals with chronic kidney disease must exercise particular caution with ALL supplements, as impaired excretion can cause accumulation and toxicity.
Always consult your physician, nephrologist, or cardiologist before beginning any supplement regimen.
Supplements are not FDA-approved treatments for CKM Syndrome.
Quality and purity vary significantly between brands — choose products with third-party testing verification (e.g., NSF, USP, Informed Sport certification).
SECTION 10
How Doctors Diagnose CKM Syndrome
There is no single blood test that diagnoses CKM Syndrome. Instead, diagnosis involves a pattern recognition process — combining clinical history, physical measurements, and a panel of laboratory tests that together paint a complete cardiometabolic and renal picture. If you are concerned about CKM risk, the following is what a comprehensive evaluation should include.
Diagnostic Assessment Framework
Test / Measurement | What It Reveals |
|---|---|
| Blood Pressure (measured correctly, at rest, both arms) | Hypertension stage, cardiovascular and renal risk stratification. Target: below 130/80 mmHg for most adults. |
| Fasting Blood Glucose | Screening for prediabetes (100–125 mg/dL) and type 2 diabetes (126+ mg/dL). Reveals baseline glycemic status. |
| HbA1c (Glycated Hemoglobin) | Reflects average blood glucose over 2–3 months. Prediabetes: 5.7–6.4%. Diabetes: 6.5%+. More reliable than fasting glucose alone. |
| Fasting Lipid Panel | Measures total cholesterol, LDL, HDL, and triglycerides. Metabolic risk pattern: high triglycerides + low HDL + small dense LDL particles. |
| eGFR (Estimated Glomerular Filtration Rate) | Estimates kidney filtration capacity. Below 60 mL/min/1.73m2 for 3+ months indicates chronic kidney disease. |
| Urine Albumin-to-Creatinine Ratio (UACR) | Detects albuminuria (protein in urine) — a critical early marker of kidney stress and an independent cardiovascular risk predictor. A UACR above 30 mg/g is clinically significant. |
| Waist Circumference | Visceral fat measurement. Risk thresholds: >94 cm in men, >80 cm in women (WHO). Metabolic risk increases substantially above these values. |
| High-Sensitivity C-Reactive Protein (hsCRP) | Marker of systemic inflammation. Elevated hsCRP (>2 mg/L) is associated with increased cardiovascular and metabolic risk. |
| Uric Acid | Elevated uric acid is associated with insulin resistance, hypertension, and kidney disease — and is increasingly recognized as a CKM marker. |
| Liver Function Tests / ALT | Elevated ALT can indicate non-alcoholic fatty liver disease (NAFLD) — increasingly recognized as a key component and predictor of cardiometabolic dysfunction. |
| Cardiovascular Risk Score (e.g., 10-year ASCVD Risk) | Integrates age, sex, cholesterol, blood pressure, diabetes status, and smoking into an estimated 10-year cardiovascular event probability — guiding treatment decisions. |
| ECG / Echocardiogram (where indicated) | Detects structural cardiac changes (left ventricular hypertrophy, valve disease, cardiomegaly) that may not yet produce symptoms. |
HOW OFTEN SHOULD YOU BE SCREENED? |
|---|
| Ages 35-44 with no risk factors: Every 2-3 years minimum. |
| Ages 35-44 with 1+ risk factor (obesity, family history, borderline readings): Annually. |
| Ages 45+ with any CKM risk factors: Annual comprehensive cardiometabolic panel. |
| Diagnosed prediabetes or CKD: Every 6-12 months as directed by your physician. |
| Note: These are general guidelines. Your physician will recommend an individualized screening schedule. |
SECTION 11
Common Mistakes People Make When Managing CKM Risk
Understanding what NOT to do is just as important as knowing the right steps to take. Many well-intentioned individuals inadvertently undermine their cardiometabolic health through avoidable errors. Recognizing these patterns is the first step to correcting them.
Common Mistake | Why It Is Problematic — and What to Do Instead |
|---|---|
| Ignoring early symptoms because they seem mild | Fatigue, mild swelling, and borderline blood pressure readings are easy to dismiss, but in the context of CKM risk, they are valuable early signals. Get screened when early signs appear, not only when symptoms become severe. |
| Waiting for a serious event (heart attack, kidney failure) before acting | CKM Syndrome is far more reversible in its early stages. By Stage 4, organ damage is often irreversible. Early action is not just advisable, it is transformative. |
| Attempting extreme crash diets | Severe caloric restriction raises cortisol, causes muscle mass loss (worsening insulin resistance), and is rarely sustainable. The target is a modest, consistent caloric reduction of 500–750 kcal/day alongside dietary quality improvements, not deprivation. |
| Treating CKM as a single condition rather than a systems problem | Focusing only on blood sugar while ignoring blood pressure and kidney markers misses the integrated nature of the syndrome. All three domains require simultaneous monitoring and management. |
| Overrelying on supplements while neglecting lifestyle | No supplement compensates for a sedentary lifestyle, poor sleep, and a high-processed-food diet. Supplements are adjuncts, not alternatives. |
| Avoiding medical checkups due to fear or cost | Delayed diagnosis is one of the most avoidable contributors to poor CKM outcomes. Many healthcare systems now offer preventive screening programs with reduced or no cost barriers, explore what is available to you. |
| Chronic poor sleep being treated as a lifestyle choice rather than a health risk | Sleep deprivation of even one hour per night, sustained over months, has measurable effects on insulin sensitivity, blood pressure, and inflammatory markers. Prioritizing sleep is a medical priority, not a luxury. |
| Doing intense exercise without warming up (with cardiovascular risk) | For individuals with established cardiovascular disease or Stage 3–4 CKM, exercise remains beneficial, but intensity must be appropriate. A supervised cardiac rehabilitation or exercise physiology consultation is valuable for those with elevated cardiac risk. |
SECTION 12
Realistic Patient Scenarios & Recovery Stories
Clinical data and guidelines are essential, but stories make the human stakes of CKM Syndrome tangible and real. The following composite scenarios are inspired by common clinical presentations. They are illustrative rather than accounts of specific individuals, and outcomes reflect what is realistic with evidence-based care and sustained lifestyle change.
Scenario 1: Marcus, 47 — The Office Worker Who Almost Missed the SignsMarcus had always considered himself reasonably healthy. He walked occasionally, ate what he thought was a balanced diet, and hadn't been to the doctor in three years. At a company-sponsored health screening, his results showed borderline blood pressure (136/86 mmHg), fasting glucose of 108 mg/dL (prediabetic), a waist circumference of 101 cm, and a triglycerides-to-HDL ratio of 5:1. His eGFR was 74 — slightly reduced but not yet alarming. His physician sat with him and explained: 'You are at Stage 2 CKM Syndrome. Nothing is broken yet, but this is a genuine warning.' With guidance from a registered dietitian and a lifestyle medicine physician, Marcus committed to a Mediterranean-style diet, a 30-minute daily walk, and a sleep schedule. Twelve months later, his fasting glucose had dropped to 95 mg/dL, blood pressure to 124/78 mmHg, and waist circumference by 9 cm. His eGFR stabilized at 78. He did not need medication. He needed a plan — and the knowledge that action was urgently possible. |
Scenario 2: Priya, 54 — Managing Diabetes and Kidney Strain TogetherPriya had been living with type 2 diabetes for six years when her nephrologist noted a declining eGFR of 55 and a UACR of 85 mg/g, early diabetic nephropathy. She was already on metformin and a blood pressure medication but acknowledged that her diet was 'not great' and that she rarely exercised. Working with a multidisciplinary CKM team (endocrinologist, nephrologist, and dietitian), Priya began a renal-friendly Mediterranean diet, started a supervised walking program, and added a SGLT2 inhibitor (a medication class with demonstrated kidney and cardiovascular protective effects). Two years later, her eGFR had stabilized at 57, her UACR had decreased to 44 mg/g, and her HbA1c had improved from 8.1% to 6.8%. Her cardiovascular risk score had meaningfully decreased. 'I thought the damage was already done,' she said. 'But my kidney numbers actually got better. That gave me a reason to keep going.' |
Scenario 3: David, 41 — Reversing Metabolic Risk Before It Became DiseaseDavid was 41 when his physician flagged his bloodwork: elevated triglycerides (310 mg/dL), low HDL (36 mg/dL), fasting glucose of 112 mg/dL, and a blood pressure trend of 132/84 over three consecutive readings. He had gained 14 kg over the previous five years, mostly working from home during the pandemic years. Rather than immediately prescribing medication, his physician suggested a 12-week intensive lifestyle program. David began intermittent resistance training, significantly reduced ultra-processed food intake, prioritized 7.5 hours of sleep, and cut alcohol from five to zero nights per week. At his 6-month review, his triglycerides had dropped to 178 mg/dL, HDL had risen to 44 mg/dL, fasting glucose normalized to 98 mg/dL, and blood pressure was consistently below 128/80 mmHg. The biology responded. It always does, when given the right conditions. |

SECTION 13
When to Seek Medical Help Immediately
Preventive care is the goal — but knowing when a symptom has crossed from 'monitor it' to 'seek help now' is equally critical. The following symptoms, particularly in the context of known CKM risk factors, require prompt medical evaluation. Do not drive yourself to the emergency room if you suspect a cardiac or neurological emergency. Call emergency services immediately.
SEEK EMERGENCY CARE IMMEDIATELY FOR:
CHEST PAIN OR PRESSURE
Especially if radiating to the arm, jaw, neck, or back. Any new or unexplained chest discomfort should be treated as a potential cardiac event until proven otherwise.
SEVERE OR SUDDEN SHORTNESS OF BREATH
Particularly at rest, on waking, or with minimal activity. This may indicate acute heart failure, pulmonary edema, or serious cardiac dysfunction.
SUDDEN WEAKNESS OR NUMBNESS
Particularly one-sided. Combined with face drooping or slurred speech, these are warning signs of stroke. Act FAST: Face, Arms, Speech, Time.
MARKED SWELLING (SEVERE EDEMA)
Rapid onset of severe swelling in the legs, ankles, or face — especially with breathlessness — may signal acute heart failure or kidney crisis.
BLOOD PRESSURE CRISIS
Readings above 180/120 mmHg with symptoms such as headache, visual changes, chest pain, or confusion require emergency evaluation.
SEVERELY UNCONTROLLED BLOOD SUGAR
Blood glucose above 300 mg/dL with symptoms, or any concern for diabetic ketoacidosis (DKA) or hyperosmolar hyperglycemic state (HHS).
SUDDEN SEVERE FATIGUE WITH CONFUSION
May indicate serious cardiac output failure, severe anemia of kidney disease, or metabolic crisis.
For symptoms that are concerning but not immediately life-threatening, such as new significant edema, unexplained persistent breathlessness, or blood pressure consistently above 160/100 mmHg — schedule an urgent medical appointment within 24–48 hours rather than waiting for a routine visit.
SECTION 14
The Future of Cardiometabolic Health
Medicine in 2026 looks fundamentally different from even five years ago, and the pace of innovation in cardiometabolic health is accelerating. From real-time metabolic monitoring to AI-assisted health prediction, the tools available for preventing and managing CKM Syndrome are becoming more precise, more accessible, and more personalized.
Emerging Technologies and Approaches
Innovation | Potential Impact on CKM Syndrome |
|---|---|
| Continuous Glucose Monitors (CGM) for Non-Diabetics | CGMs are now available for use by individuals at metabolic risk, not just those with diagnosed diabetes. Real-time glucose data helps identify food sensitivities, postprandial spikes, and lifestyle patterns that standard fasting labs miss entirely. |
| Wearable Cardiometabolic Monitors | Next-generation smartwatches and patches can continuously track heart rate variability (HRV), blood pressure trends, oxygen saturation, and sleep architecture, providing a continuously updated cardiometabolic risk picture. |
| AI-Assisted Health Risk Prediction | Machine learning models trained on large cardiometabolic datasets are being deployed to identify CKM Syndrome progression risk years before clinical thresholds are met, enabling proactive intervention at a population scale. |
| SGLT2 Inhibitors and GLP-1 Receptor Agonists | These medication classes, originally developed for diabetes, have demonstrated remarkable cardiovascular and kidney-protective effects independent of glycemic control, transforming the treatment landscape for CKM Syndrome. |
| Precision Nutrition and Nutrigenomics | Tailored dietary recommendations based on individual genetic variants, microbiome profiles, and metabolic phenotyping are moving from research to clinical practice, enabling CKM prevention strategies personalized to your biology. |
| Telehealth and Digital Therapeutics | Remote monitoring platforms allow physicians to track CKM metrics between appointments in real time, enabling earlier intervention without requiring in-person visits for every data point. |
| Inflammation Biomarker Panels | Expanded inflammatory marker testing (beyond CRP), including IL-6, TNF-alpha, and oxidized LDL, is enabling more precise identification of individuals at high CKM risk who would be missed by conventional lipid and glucose panels. |
| Longevity Medicine and Integrated Metabolic Care | A growing movement in preventive and longevity medicine is treating CKM Syndrome not merely as a disease-risk cluster but as a biological aging accelerator, integrating mitochondrial health, cellular senescence, and metabolic optimization into comprehensive cardiometabolic care. |
"The future of CKM care is personalized, predictive, and proactive. The best time to begin is always now, because the biology of prevention is most powerful before the damage becomes irreversible."
SECTION 15
Conclusion: Prevention Is Power
CKM Syndrome is real, it is widespread, and for millions of people it is developing silently right now, undetected, unnamed, and unaddressed. But it is not inevitable. It is not irreversible in its early stages. And it is not beyond your ability to influence.
The three organs at the center of CKM Syndrome, the heart, the kidneys, and the metabolic system, are remarkably responsive to the right inputs. Sleep. Movement. Real food. Stress reduction. Medical monitoring. These are not radical interventions. They are the biological conditions your body was always designed to function within.
What has changed is our environment, a world of ultra-processed convenience, digital sedentarism, chronic stress, and fragmented sleep. Reclaiming your cardiometabolic health in 2026 is, in many ways, an act of conscious counter-culture. It requires intention, but it does not require perfection.
The most powerful message in all of preventive medicine is simple: you are not too late. If you are reading this article and recognizing warning signs, you have already taken the most important step, awareness. From awareness flows understanding. From understanding flows action. And from consistent, small, daily actions flows the kind of biological transformation that standard medicine sometimes calls extraordinary, but that is, in truth, simply the body doing what it has always been capable of, given the right conditions.
Talk to your doctor. Get your numbers. Make one change this week. Then another next week. The 2026 you that is reading this deserves a healthier, longer, more energetic life. The biology is on your side. The science is on your side. And now, so is the knowledge.
TAKE THE FIRST STEP TODAY
1. Schedule a comprehensive cardiometabolic screening with your healthcare provider. 2. Start a 20-minute daily walk this week. 3. Replace one ultra-processed food with a whole-food alternative each day. 4. Prioritize 7 hours of sleep starting tonight. 5. Share this article with someone you care about who may benefit. Your CKM prevention journey begins with a single, informed decision.
FAQ Frequently Asked Questions About CKM Syndrome
Q: What is CKM Syndrome in simple terms?
A: CKM Syndrome is a medical term for the interrelated cluster of conditions, cardiovascular (heart) disease, kidney disease, and metabolic dysfunction (obesity, diabetes, insulin resistance), that tend to develop together and worsen one another. It is not a single disease but a systems-level health challenge requiring integrated prevention and management.
Q: Can CKM Syndrome be reversed?
A: In its early stages (Stages 0–2), the progression of CKM Syndrome can often be significantly slowed or halted, and in some cases, key markers can meaningfully improve, through sustained lifestyle change and appropriate medical management. By Stage 3 and 4, organ damage may be partially irreversible, though lifestyle change and medication can still dramatically reduce risk and improve quality of life. Early action produces the best outcomes.
Q: Do I need to see a specialist for CKM Syndrome?
A: Your primary care physician or general practitioner is the appropriate starting point for screening and early-stage management. Depending on findings, you may be referred to specialists including a cardiologist (heart), nephrologist (kidneys), endocrinologist (diabetes/metabolism), or a lifestyle medicine physician who integrates all three domains.
Q: Is CKM Syndrome the same as metabolic syndrome?
A: Metabolic syndrome is a related but narrower cluster of findings (central obesity, high blood pressure, high fasting glucose, high triglycerides, low HDL). CKM Syndrome is broader, it explicitly includes kidney disease and cardiovascular disease as active components, and it frames the interconnection between these domains as a unified clinical syndrome requiring integrated care.
Q: What is the best diet for CKM Syndrome?
A: The Mediterranean dietary pattern, emphasizing whole grains, legumes, vegetables, fruits, fish, and olive oil while limiting processed foods, added sugars, and excess sodium, has the strongest evidence base for reducing cardiovascular, renal, and metabolic risk simultaneously. The DASH diet is also highly evidence-backed, particularly for blood pressure management.
Q: How can I tell if I am at risk for CKM Syndrome?
A: Key risk indicators include: age 35+, overweight or obesity (especially central), elevated blood pressure, elevated fasting glucose or HbA1c, high triglycerides or low HDL, family history of heart disease, diabetes, or kidney disease, and a sedentary lifestyle. If you have two or more of these, a comprehensive cardiometabolic screening is strongly recommended.
Q: Are there specific medications for CKM Syndrome?
A: There is no single 'CKM Syndrome medication,' but several drug classes now have evidence supporting protective effects across multiple CKM domains simultaneously. These include SGLT2 inhibitors (cardio- and nephroprotective with glucose-lowering effects) and GLP-1 receptor agonists (cardiovascular risk reduction, weight loss, metabolic improvement). Discuss evidence-based medication options with your physician based on your specific profile.
Q: How does sleep affect CKM Syndrome?
A: Sleep is foundational to cardiometabolic health. Chronic sleep deprivation (under 7 hours) is independently associated with increased insulin resistance, elevated blood pressure, higher inflammatory markers, and greater visceral fat accumulation, all key drivers of CKM Syndrome progression. Prioritizing 7–9 hours of quality sleep is not optional; it is a core metabolic health intervention.
AL MEDIA
Trusted Health Resource Recommendations
The following organizations and resources provide evidence-based, publicly available information on cardiovascular, kidney, and metabolic health. We recommend these for further reading and self-education:
Organization / Resource | What They Offer |
|---|---|
| American Heart Association (heart.org) | Cardiovascular health education, clinical guidelines, CKM Syndrome resources, diet guides, and heart-health risk calculators. |
| National Kidney Foundation (kidney.org) | Kidney disease education, eGFR calculators, CKD staging information, dietary guidance for renal health. |
| American Diabetes Association (diabetes.org) | Comprehensive diabetes and prediabetes resources, nutrition guidance, clinical standards, and lifestyle tools. |
| Centers for Disease Control and Prevention, Diabetes Prevention Program (cdc.gov/diabetes) | Evidence-based lifestyle change program for prediabetes prevention, offered across the US and internationally. |
| NIDDK — National Institute of Diabetes and Digestive and Kidney Diseases (niddk.nih.gov) | In-depth, clinically reviewed information on metabolic and kidney health for patients and professionals. |
| PubMed / Cochrane Reviews (pubmed.ncbi.nlm.nih.gov) | For readers who want to explore the primary scientific literature on CKM Syndrome, metabolic health, and clinical trials. |
IMPORTANT DISCLAIMER: This article is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional regarding any questions you may have about your health, symptoms, or medical conditions. Never disregard professional medical advice or delay seeking it because of information you have read in this article. The author and publisher expressly disclaim responsibility for any adverse effects arising from the use or application of information contained herein.