1. When the World Goes Quiet But Your Mind Won't Stop
It starts subtly. You walk into the kitchen and forget why you came. You open an email you have read three times and cannot absorb a single sentence. You sit in a meeting, a meeting you have run confidently for fifteen years, and you feel, unneringly, like a stranger in your own mind.
You are not losing your intelligence. You are not developing dementia. You are not imagining it. What you are experiencing has a name: menopause brain fog. And for millions of women between the ages of 40 and 60, it is one of the most disorienting, frustrating, and least-discussed aspects of hormonal transition.
Then come the nights. You fall asleep exhausted and wake at 3 a.m., heart pounding, sheets damp with sweat. The next day, you move through the hours as though walking through water, heavy, slow, disconnected. Your mood shifts faster than you can track. You cry in the car and cannot quite explain why. You snap at the people you love most, then feel an awful wave of guilt that you cannot shake.
This is the reality of perimenopause and menopause for a remarkable number of women. And yet, when many of those women finally sit across from a doctor and describe what they are experiencing — the fog, the heat, the mood swings, the exhaustion — they are still far too often told: this is normal. Or: it will pass. Or, quietly devastating: there is not much we can do.
"I felt like my brain had a dial, and someone had turned it down to half-power. I wasn't sad exactly, I just wasn't fully there." — A composite experience shared by thousands of perimenopausal women
But something significant is shifting in women's healthcare, and it is long overdue.
After two decades of hesitation, fear, and insufficient guidance, estrogen therapy is undergoing a major scientific re-evaluation. Researchers, menopause specialists, and women's health advocates are revisiting earlier findings, examining new data, and arriving at a more nuanced, more hopeful, and more personalised understanding of hormonal treatment options.
This guide is for you, the woman who googles her symptoms at midnight, who has printed out conflicting articles and still has no clear answers, who deserves both scientific truth and genuine compassion. We will walk through what the evidence actually says in 2026, clearly, honestly, and without ideology.
Because you deserve information that respects your intelligence and your wellbeing equally.
2. What Is Menopause Brain Fog and Why Does It Happen?
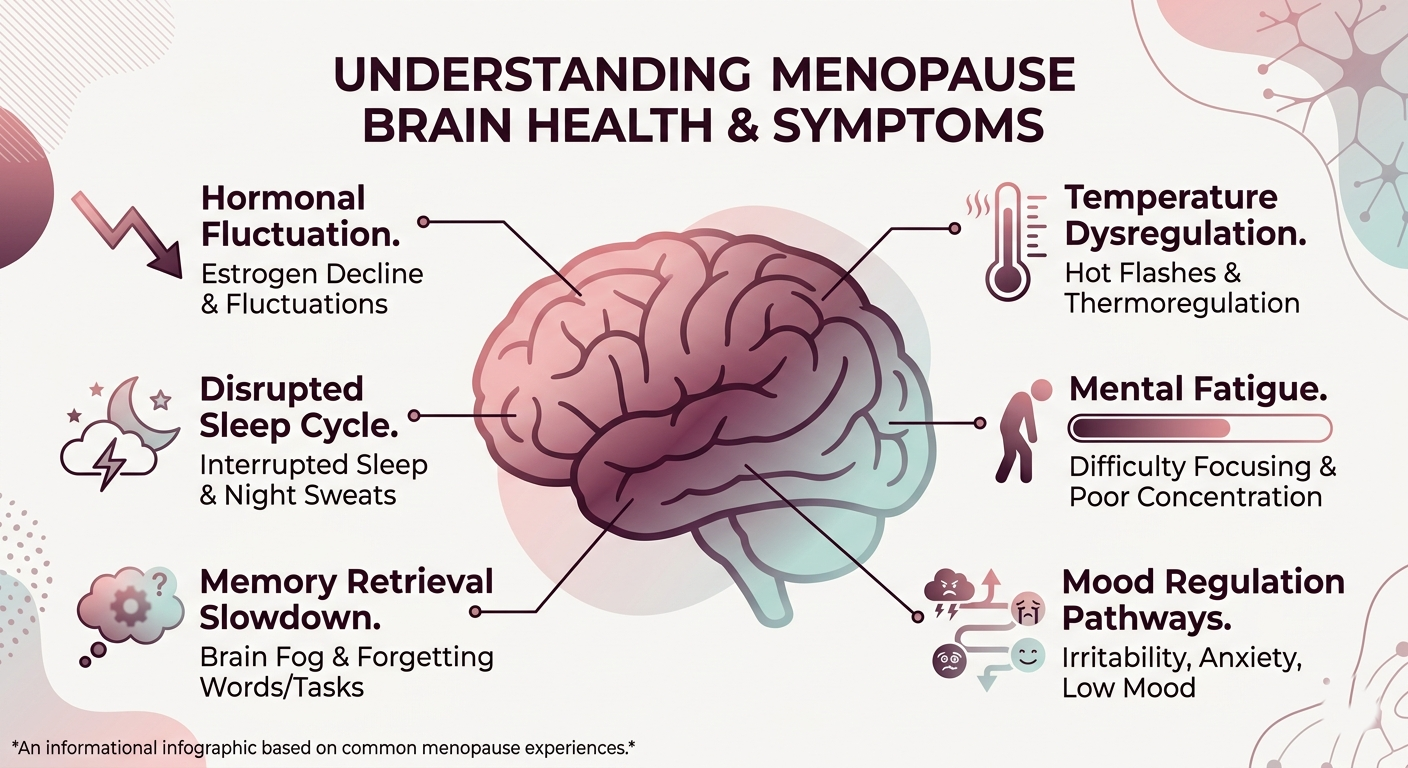
Brain fog is one of the most common yet chronically underrecognised symptoms of menopause. It is not one single experience but a cluster of cognitive changes that can include:
Difficulty concentrating or sustaining attention
Memory lapses — forgetting words, names, or what you were doing
Slower processing speed and mental sluggishness
Difficulty learning new information or retaining it
Increased mental fatigue, especially under stress
Feeling emotionally overwhelmed, disconnected, or mentally 'flat'
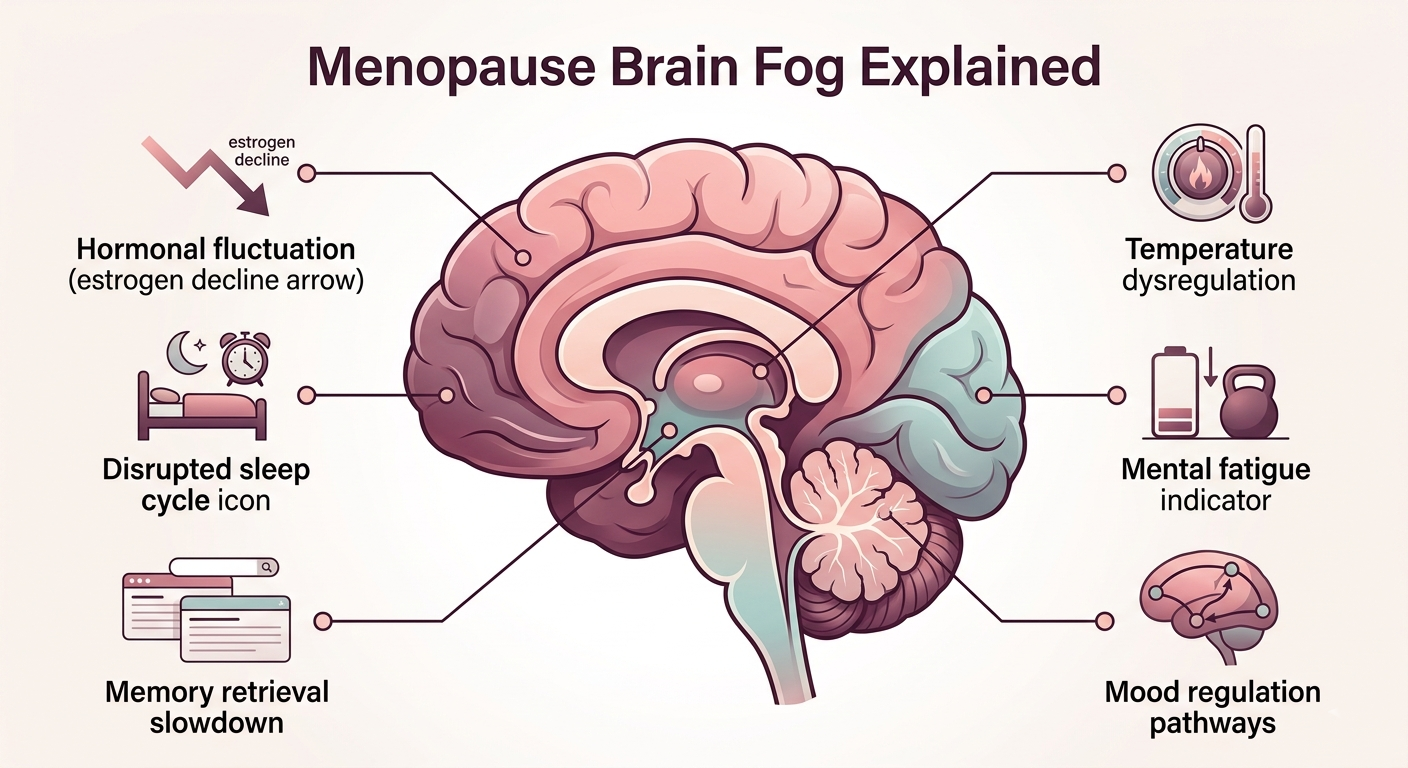
The Hormone–Brain Connection
Estrogen does far more in the body than most people realise, including in the brain. Oestrogen receptors are found throughout the brain, including in areas critical to memory, mood, and executive function: the hippocampus, the prefrontal cortex, and the limbic system.
When estrogen levels begin to fluctuate, as they do in perimenopause, often years before the final menstrual period, these brain regions feel it. Estrogen supports the production and action of neurotransmitters including serotonin, dopamine, and acetylcholine, all of which play roles in mood, focus, motivation, and memory.
As estrogen fluctuates and eventually declines, so too can these neurological functions. Sleep disturbances amplify the effect: poor sleep impairs memory consolidation, reduces cognitive resilience, and fuels emotional dysregulation. It becomes a compounding cycle.
Is Brain Fog Permanent?
Research suggests that for many women, cognitive symptoms are most pronounced during perimenopause, the transitional phase, and often improve or stabilise following menopause. However, the experience is highly individual. Some women sail through with minimal cognitive disruption. Others describe years of significant impairment affecting their professional performance, relationships, and sense of self.
The good news: cognitive symptoms during menopause are increasingly understood as a treatable component of hormonal transition, not an inevitable, irreversible decline.
Brain fog in menopause is not a sign of weakness or cognitive failure. It is a neurological response to hormonal change, and it can be addressed.
3. Why Estrogen Therapy Is Making a Comeback
To understand why estrogen therapy is being reconsidered, it helps to understand why it fell out of favour in the first place.
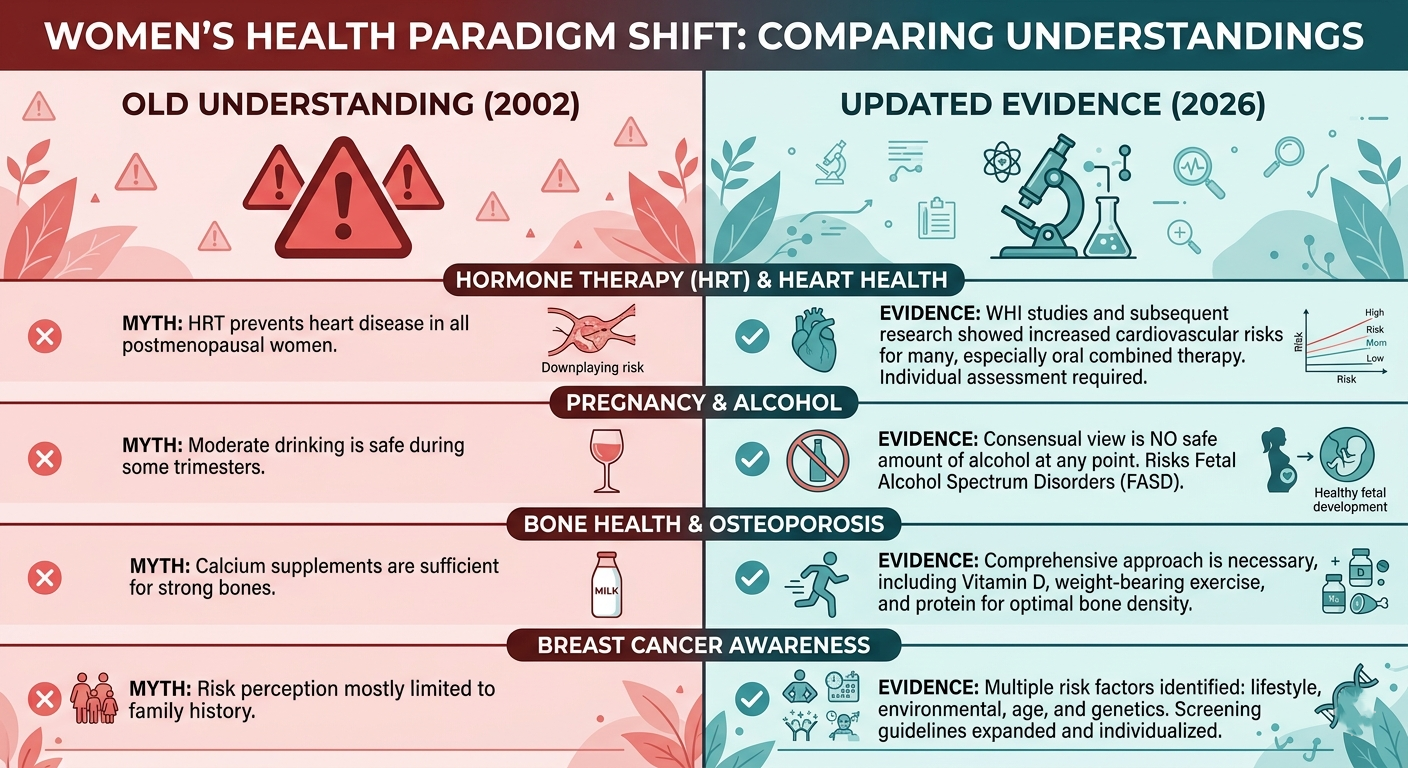
The 2002 WHI Study and What It Got Wrong
In 2002, the Women's Health Initiative (WHI) published findings that sent shockwaves through women's healthcare. The study, which examined a combined oestrogen-progestogen therapy in a large group of post-menopausal women, reported increased risks of breast cancer, stroke, and cardiovascular disease. Almost overnight, millions of women stopped taking HRT. Prescriptions plummeted. Fear became the dominant framework.
But as subsequent analysis revealed, the original WHI findings came with significant caveats that were not fully communicated to the public or, in many cases, to prescribing doctors.
The average age of participants was 63, well past early menopause. Many had gone over a decade without hormones before starting the study.
The study used oral conjugated equine oestrogen combined with medroxyprogesterone acetate, a specific formulation and delivery method that may not reflect modern approaches.
The findings were applied broadly to all women on all forms of HRT, a generalisation that subsequent researchers have challenged.
The absolute risk increases, for many women, were smaller than initial headlines suggested.
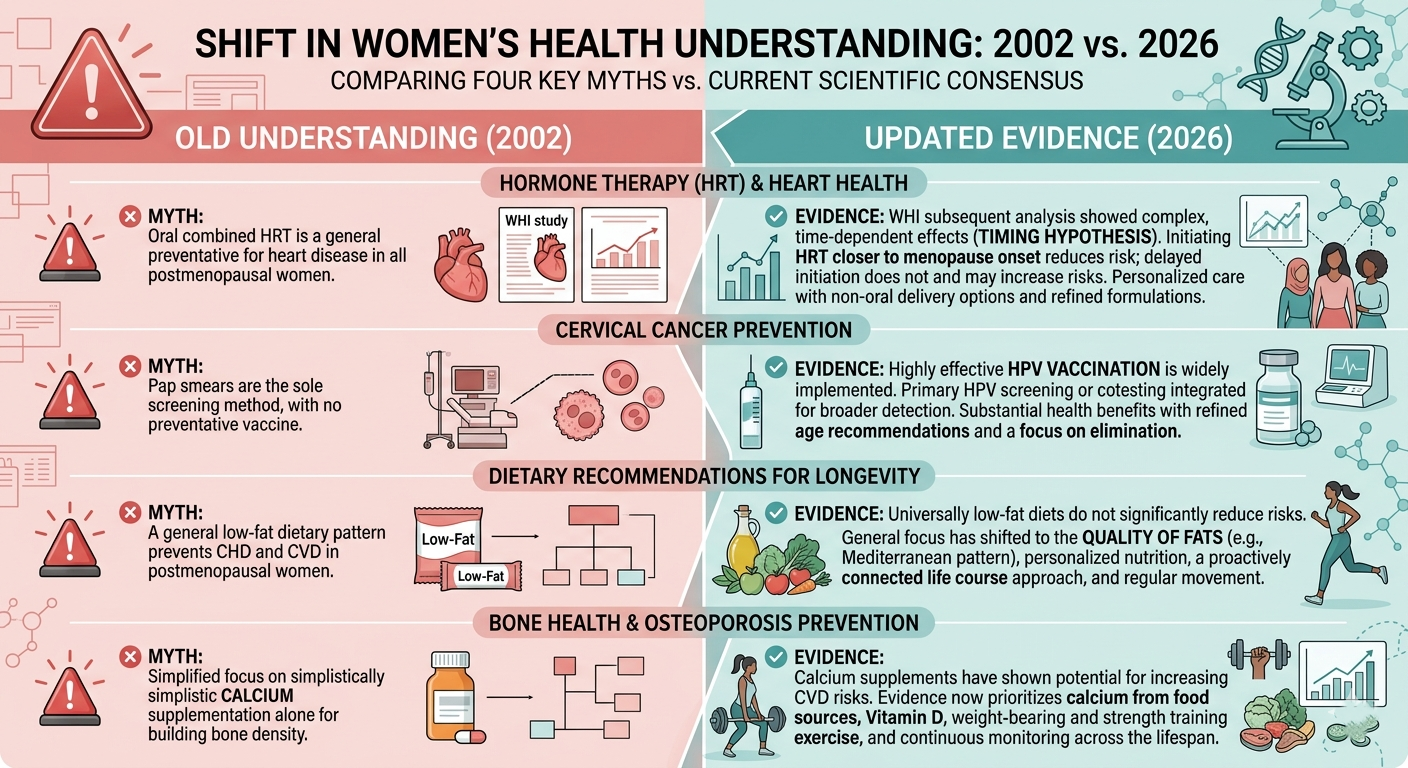
The Timing Hypothesis: A Critical Shift
Perhaps the most significant development in HRT research since 2002 is what has become known as the 'timing hypothesis', or the 'window of opportunity.' Research suggests that initiating hormone therapy closer to the onset of menopause (typically before age 60 or within 10 years of the final menstrual period) may offer different risk profiles and potential cardiovascular benefits compared to initiating therapy much later in life.
This does not mean hormone therapy is universally safe or appropriate, individual factors remain paramount. But it does mean that the conversation is now considerably more nuanced than 'hormones cause cancer.'
Key Research Update — 2026 PerspectiveMajor menopause societies, including the Menopause Society (formerly NAMS), the British Menopause Society, and the International Menopause Society, have updated their guidelines to reflect a more individualised, risk-stratified approach to HRT. Many now state that for healthy women under 60, or within 10 years of menopause, the benefits of hormone therapy for symptom relief generally outweigh the risks. This represents a meaningful departure from the blanket caution that dominated the 2000s and 2010s. |
The Role of Delivery Method and Formulation
Modern hormone therapy is not the same as the therapies used in 2002. The development of transdermal (patch, gel, spray) delivery methods, lower doses, and micronised progesterone has changed the risk-benefit calculation for many women. Transdermal estradiol, for example, does not appear to carry the same elevated blood clot risk as oral oestrogen, a clinically meaningful distinction.
4. What Estrogen Actually Does in Your Body
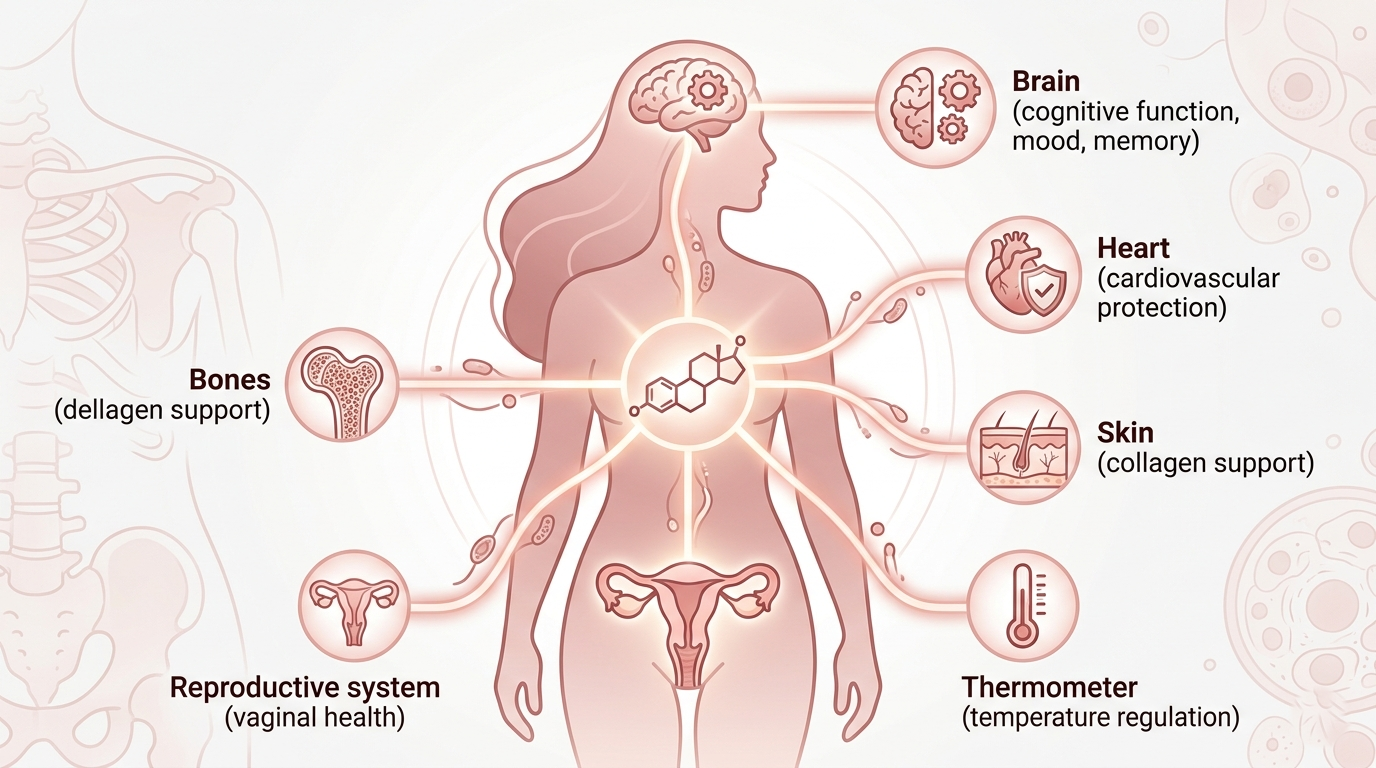
Estrogen is often described narrowly as a 'reproductive hormone,' but its reach extends throughout almost every system in the female body. Understanding this scope helps explain why its decline during menopause can produce such wide-ranging symptoms.
Brain Health and Cognition
Estrogen supports the production of acetylcholine, a neurotransmitter essential to learning and memory. It also modulates serotonin and dopamine pathways, which is why estrogen fluctuations can dramatically affect mood, motivation, and emotional regulation. Estrogen promotes neuroplasticity and may have neuroprotective effects, which is why its role in cognitive aging is an active area of research.
Mood Regulation
The connection between estrogen and mood is well-established. Serotonin receptors are sensitive to estrogen levels, and the mood disruptions many women experience during perimenopause, irritability, anxiety, low mood, emotional volatility, are closely linked to hormonal fluctuation rather than purely psychological factors.
Sleep Quality
Estrogen supports healthy sleep architecture by regulating body temperature and working alongside progesterone, which has natural sedative-like properties. Night sweats and hot flashes, direct results of temperature dysregulation, fragment sleep. Progesterone's decline adds further disruption. Poor sleep, in turn, amplifies every other menopausal symptom.
Bone Health
Estrogen is critical to bone density regulation. It inhibits the cells (osteoclasts) that break down bone tissue and supports those (osteoblasts) that build it. The accelerated bone loss that occurs in the first several years following menopause is directly linked to estrogen decline, making post-menopausal osteoporosis a significant women's health concern and a well-established indication for hormone therapy in appropriate candidates.
Cardiovascular Health
In younger women, estrogen appears to have a beneficial effect on cardiovascular risk markers, including LDL and HDL cholesterol, blood vessel flexibility, and inflammatory pathways. This cardioprotective effect diminishes as estrogen declines, which helps explain why cardiovascular disease risk rises significantly in women after menopause.
Temperature Regulation
The hypothalamus, the brain's thermostat, is highly sensitive to estrogen. As levels decline, the body's temperature-regulation system becomes unstable — producing the hot flashes and night sweats that are among the most recognisable menopause symptoms.
Vaginal and Sexual Health
Estrogen maintains the health and moisture of vaginal tissue. Its decline causes genitourinary syndrome of menopause (GSM), characterised by vaginal dryness, discomfort, urinary symptoms, and changes in sexual comfort. This is a condition that responds well to localised estrogen therapy and often improves significantly with targeted treatment.
5. Common Symptoms of Perimenopause and Menopause
Perimenopause, the transitional phase leading up to menopause, can begin as early as the mid-30s but most commonly in the mid-40s. It can last anywhere from two to twelve years. Menopause itself is defined as 12 consecutive months without a menstrual period. The symptoms below can occur across both phases.
Perimenopause & Menopause Symptom Checklist | |
|---|---|
| ☐ Brain fog and poor concentration | ☐ Low libido |
| ☐ Memory lapses and word-finding difficulty | ☐ Vaginal dryness and discomfort |
| ☐ Hot flashes and heat surges | ☐ Joint pain and muscle aches |
| ☐ Night sweats | ☐ Weight changes and metabolic shifts |
| ☐ Sleep disturbance and insomnia | ☐ Hair thinning or texture changes |
| ☐ Anxiety and restlessness | ☐ Skin dryness and changes |
| ☐ Low mood or depression | ☐ Headaches or migraines |
| ☐ Irritability and emotional volatility | ☐ Urinary symptoms and urgency |
| ☐ Fatigue and low energy | ☐ Bloating and digestive changes |
| ☐ Heart palpitations | ☐ Reduced confidence and motivation |
If you are experiencing five or more of the above symptoms and are between the ages of 38 and 60, it is worth having a conversation with your doctor or a menopause specialist. You do not need to manage this alone.
Important Note
Symptoms vary enormously between individuals. Some women experience minimal disruption; others describe profound impact on every area of their lives. There is no 'normal' menopause, only your menopause. This is exactly why personalised care matters.
6. Is Estrogen Therapy Safe in 2026?
This is the question every woman searching these topics eventually lands on, and it deserves a direct, honest answer.
The short answer: estrogen therapy is not universally safe, and it is not universally unsafe. It is a medical treatment with a specific risk-benefit profile that depends significantly on the individual. The right answer for you depends on your age, health history, symptom burden, values, and access to qualified medical guidance.
Here is what the updated science suggests:
| Common HRT Myth | What Updated Evidence Actually Shows |
|---|---|
| HRT always causes breast cancer | The relationship is nuanced. Risk depends on type, duration, and individual factors. Estrogen-only therapy has a different profile from combined therapy. For many women, absolute risk increases are small. |
| HRT is dangerous for the heart | For women who begin therapy before age 60 or within 10 years of menopause, evidence does not support increased cardiovascular risk and may suggest benefit in some cases. |
| All HRT is the same | Formulation, delivery method, dose, and type differ significantly. Transdermal estradiol has a different clot-risk profile than oral oestrogen. Bioidentical micronised progesterone differs from synthetic progestins. |
| You should stop as soon as possible | Duration should be individualised. Many specialist guidelines now support continuing therapy as long as the woman and her clinician feel benefits outweigh risks, with regular review. |
| Natural menopause is always healthier | Untreated severe menopause symptoms carry their own health consequences, sleep deprivation, bone loss, cardiovascular changes, and quality-of-life deterioration all represent real health risks. |
The Timing Hypothesis in Practice
The timing hypothesis, that initiating hormone therapy closer to menopause onset confers different risk and benefit profiles than initiating it a decade or more later, has become one of the most influential frameworks in menopause medicine. Evidence suggests that women who begin therapy in the early post-menopausal period may experience cardiovascular benefit, while those who begin very late may not, and may face different risks.
This has led to updated guidance encouraging women to consider therapy sooner rather than delaying until symptoms become severe, while still emphasising the importance of individual clinical assessment.
Who Should Be Cautious or Avoid HRT
Estrogen therapy is not appropriate for all women. Those who should discuss alternative options with their doctor include:
Women with a personal history of hormone-receptor-positive breast cancer
Women with a history of blood clots (deep vein thrombosis or pulmonary embolism)
Women with active or recent cardiovascular disease
Women with unexplained vaginal bleeding
Women with certain clotting disorders
This is not an exhaustive list. An individualised conversation with a qualified clinician, ideally a menopause specialist, is essential before making any treatment decision.
7. Potential Benefits of Estrogen Therapy
For women who are appropriate candidates, estrogen therapy can offer meaningful improvements across multiple dimensions of health and quality of life.
| Potential Benefit | What Research Suggests |
|---|---|
| Brain Fog & Cognition | Many women report improved mental clarity, memory, and concentration. Research suggests estrogen supports neurological pathways involved in cognition, particularly when therapy is initiated around menopause. |
| Hot Flashes & Night Sweats | Hormone therapy remains the most effective treatment for vasomotor symptoms. For women with moderate-to-severe hot flashes, improvement can be substantial and rapid. |
| Mood Stability | Estrogen therapy can help stabilise mood, reduce anxiety, and alleviate low mood that is hormonally driven, particularly during perimenopause when fluctuations are most pronounced. |
| Sleep Quality | By reducing night sweats and supporting neurological sleep regulation, hormone therapy can significantly improve sleep, with cascading positive effects on energy, cognition, and mood. |
| Bone Density | Estrogen therapy is one of the most effective interventions for preventing post-menopausal bone loss and reducing fracture risk, a significant benefit for women at elevated osteoporosis risk. |
| Vaginal & Sexual Health | Local or systemic estrogen therapy can restore vaginal tissue health, reducing dryness, discomfort, and urinary symptoms, with positive effects on sexual wellbeing and intimacy. |
| Cardiovascular Markers | In appropriate candidates initiating therapy early in menopause, some studies suggest beneficial effects on cholesterol profiles and vascular health. |
| Quality of Life | For women experiencing severe menopause symptoms, the overall quality-of-life improvement from effective treatment is difficult to overstate, affecting work performance, relationships, mental health, and self-perception. |
Quality of life is not a luxury metric. Sleep, mental clarity, emotional stability, and physical comfort are the foundations of every other health outcome.
8. Potential Risks and Who Should Be Cautious
Medical responsibility requires that any discussion of estrogen therapy include an honest account of the risks. The following represent the key areas of concern, with an evidence-based framing of what is currently understood.
Breast Cancer
This is the risk that most women think of first, and it requires careful context. The risk varies by type of therapy: combined estrogen-progestogen therapy is associated with a small increased risk of breast cancer with prolonged use (5+ years). Estrogen-only therapy (for women who have had a hysterectomy) may actually be associated with a reduced risk of breast cancer in some studies, though this remains under investigation.
The absolute risk increase for individual women is often smaller than perceived, but it is real and should be weighed carefully, particularly for women with additional risk factors such as family history or BRCA gene variants. Micronised progesterone may carry a lower risk than synthetic progestins, though evidence continues to accumulate.
Blood Clots (VTE)
Oral estrogen therapy is associated with an increased risk of venous thromboembolism (blood clots). Transdermal estradiol (patch, gel, or spray) does not appear to carry the same risk, a clinically significant distinction that often informs prescribing decisions for women at elevated VTE risk.
Stroke
Some forms of oral hormone therapy have been associated with a small increase in stroke risk. Again, transdermal delivery methods appear to have a different and more favourable profile. Age, blood pressure, and smoking status are important factors in individual risk assessment.
Cardiovascular Disease
The relationship between hormone therapy and cardiovascular health is complex. As outlined under the timing hypothesis, initiating therapy early in menopause may be cardioprotective for many women, while initiating it later, or in women with existing cardiovascular disease, may not be safe or appropriate.
Bottom Line on Risk
Risks are real, variable, and highly individual. Many women's absolute risk increases are smaller than they fear, but some women do have meaningfully elevated risk profiles that make alternative approaches more appropriate. This is precisely why individualised assessment with a qualified clinician is non-negotiable. There is no one-size-fits-all answer.
9. Types of Hormone Therapy: Understanding Your Options
One of the most important advances in modern menopause care is the recognition that 'HRT' is not a single treatment but a spectrum of options, varying by hormone type, formulation, delivery method, and dose. Here is a clear overview:
By Hormone Composition
Estrogen-Only Therapy:
Used for women who have had a hysterectomy. Avoids the need for progesterone. Generally considered to have a different and in some respects more favourable risk profile than combined therapy.
Combined Estrogen-Progestogen Therapy:
For women with an intact uterus. Progesterone is added to protect the uterine lining from the effects of unopposed estrogen. The type of progestogen used matters, micronised progesterone is increasingly preferred over older synthetic progestins.
By Delivery Method
| Delivery Method | Key Characteristics & Considerations |
|---|---|
| Oral tablets | Convenient and familiar. Systemic effect. Some elevation in blood-clot risk with oral estrogen. Generally taken daily. |
| Transdermal patches | Absorbed through the skin. Avoids first-pass liver metabolism. Does not appear to carry the elevated clot risk of oral estrogen. Changed 1-2 times per week. |
| Gel or spray | Applied to skin daily. Transdermal; similar advantages to patches in terms of clot risk. Dose easily adjustable. Popular for flexibility. |
| Vaginal estrogen (cream, ring, tablet) | Local treatment for genitourinary symptoms — vaginal dryness, discomfort, urinary urgency. Minimal systemic absorption. Generally considered safe even for many women who cannot use systemic therapy. |
| Implants/pellets | Inserted under the skin. Long-lasting. Less commonly used in mainstream practice. |
| Vaginal ring (systemic) | Releases systemic estrogen. Different from purely local vaginal rings. Used for broader symptom management. |
Bioidentical Hormones — What the Term Actually Means
'Bioidentical' refers to hormones that are structurally identical to those naturally produced by the body. FDA-approved bioidentical options (such as estradiol patches and micronised progesterone) are available and are what many menopause specialists mean when they discuss modern HRT. Compounded bioidentical hormones, customised formulations from specialist pharmacies, are also used but carry less regulatory oversight and standardisation, and their safety data is more limited.
The term 'bioidentical' is sometimes used in direct-to-consumer marketing in ways that can be misleading. Discuss with your doctor what 'bioidentical' means in the context of your specific prescription.
10. Natural and Lifestyle Approaches That May Help
Hormone therapy is not the only tool available for managing menopause symptoms, and for many women, lifestyle approaches provide meaningful relief on their own or alongside medical treatment. None of the following replaces professional medical guidance, but all are supported by evidence and worth exploring.
Nutrition
Diet can significantly influence the experience of menopause. Key considerations include:
Increasing calcium and vitamin D intake for bone health (dairy, leafy greens, fortified foods, sunlight)
Consuming phytoestrogen-rich foods: soy, flaxseed, lentils — which may modestly reduce hot flash frequency in some women
Prioritising protein to support muscle maintenance and metabolic health
Reducing alcohol, caffeine, and spicy foods, which can trigger or worsen hot flashes in susceptible women
Following an anti-inflammatory dietary pattern (Mediterranean-style diet) for cardiovascular and cognitive benefits
Strength Training
Resistance exercise is one of the most impactful lifestyle interventions for menopausal women. It supports bone density, maintains muscle mass (which declines with age and estrogen loss), improves insulin sensitivity and metabolic health, boosts mood through endorphin release, and may improve sleep quality. Aim for at least two sessions per week.
Sleep Optimisation
Improving sleep hygiene can meaningfully support menopausal symptom management. Key strategies include keeping a consistent sleep schedule, maintaining a cool sleeping environment, reducing screen exposure before bed, limiting alcohol (which fragments sleep architecture despite feeling sedating), and considering magnesium supplementation, which some women find helpful for sleep and muscle relaxation.
Stress Reduction
Chronic stress elevates cortisol, which can worsen hormonal disruption, sleep impairment, and cognitive symptoms. Mindfulness-based stress reduction (MBSR), breathing practices, nature exposure, journalling, and therapy can all play meaningful supportive roles. Prioritising stress management is not self-indulgence, it is a health intervention.
Supplements Worth Discussing with Your Doctor
Magnesium:
May support sleep, anxiety, and muscle symptoms
Omega-3 fatty acids:
Anti-inflammatory; may support mood and cardiovascular health
Vitamin D and K2:
Bone health in combination with calcium
Ashwagandha:
Some evidence for cortisol regulation and stress resilience
Black cohosh:
Most researched botanical for hot flashes; evidence is mixed but it may help some women
Important Supplement Note
Supplements are not regulated to the same standard as medications. Always inform your doctor of any supplements you take, some interact with medications or are contraindicated in certain health conditions. 'Natural' does not automatically mean safe or effective.
Cognitive Support Strategies
For brain fog specifically, several behavioural strategies can help: externalising memory (structured lists, calendars, notes), chunking tasks into smaller units, building in regular cognitive breaks, protecting sleep ferociously, and reducing multitasking. Cognitive behavioural therapy (CBT) adapted for menopause is an evidence-based option for both cognitive symptoms and menopause-related anxiety and low mood.
11. Questions to Ask Your Doctor
Many women leave medical appointments feeling they have not had the conversation they needed. Arriving prepared makes an enormous difference. Here is a checklist of questions to bring to your next appointment:
Your Menopause Appointment ChecklistAbout Your Symptoms
About Estrogen Therapy Specifically
About Alternatives
|
12. Real Women, Real Experiences: Four Composite Stories

Sarah, 48 — The Professional Who Lost Her Edge
Sarah had been a senior project manager for twenty years. She was sharp, organised, reliable. Then, at 47, something shifted. She began losing track of conversations mid-sentence. She missed a deadline — her first in a decade, because she had simply forgotten it. She started writing everything down, convinced she was developing early dementia.
Her GP initially attributed her symptoms to work stress. It was only after she found a menopause specialist and described the full picture, the brain fog, the erratic periods, the 3 a.m. wake-ups — that she received a clinical picture that made sense. A trial of transdermal estradiol, after careful risk assessment, produced gradual but meaningful improvement in her cognitive clarity over three months. 'I feel like the lights have come back on,' she said.
Diane, 51 — The Emotional Rollercoaster
Diane described herself as 'not a crier', a calm, steady person known for emotional resilience. At 50, she began experiencing unpredictable emotional swings that frightened her. She would feel fine at breakfast and in tears by midday, without understanding why. She withdrew from social situations to avoid what she called 'the unpredictability of myself.'
After investigation, Diane's clinician identified perimenopausal hormonal fluctuation as a likely contributor. Rather than systemic hormone therapy (which she was cautious about given a first-degree relative with breast cancer), she and her doctor explored CBT for menopause and a low-dose SSRI, a non-hormonal option with evidence for menopausal mood symptoms. Over time, her emotional landscape stabilised. 'I am not fixed,' she said. 'But I understand myself again.'
Miriam, 54 — Finding the Right Fit
Miriam tried three different HRT preparations before finding one that worked. The first caused irregular spotting. The second gave her persistent headaches. The third, a gel combined with micronised progesterone, worked well. Her hot flashes reduced significantly within six weeks. Her sleep improved enough that she stopped falling asleep in front of the television every evening.
Her experience underscores an important reality: finding the right treatment approach often takes time, adjustment, and an open dialogue with a clinician who is willing to iterate. Persistence, she says, was the most important part of the process.
Clare, 49 — Choosing the Lifestyle Route
Clare was not a candidate for hormone therapy, she had a history of blood clots and was advised to consider alternative options. Initially devastated by this news, she worked with her GP and a menopause health coach to build a comprehensive lifestyle plan: strength training three times a week, a Mediterranean-style diet, a structured sleep protocol, and weekly mindfulness practice. She also began vaginal estrogen for localised symptoms, which her doctor confirmed was appropriate for her situation despite systemic contraindications.
'I won't pretend it has been effortless,' Clare says. 'But I've been surprised by how much difference intentional lifestyle changes have made. Not perfect — but manageable.'
13. The Emotional Side of Menopause — What Nobody Tells You
The physical symptoms of menopause are increasingly discussed — but the emotional and identity dimensions remain, for many women, profoundly isolating.
The Invisible Shift
Many women describe a gradual, disorienting sense of becoming invisible, in their workplaces, in social spaces, and sometimes in their own relationships. Cultural narratives around menopause, where they exist at all, often frame it as a loss: of fertility, of youth, of a particular kind of social currency. These narratives are damaging, and they are being actively challenged, but they still shape many women's internal experience of this transition.
Relationship Stress
Menopause symptoms do not occur in a vacuum. Partners who do not understand hormonal fluctuation may interpret irritability as personal grievance, withdrawal as loss of affection, and brain fog as carelessness. The relational impact of untreated menopause symptoms is underresearched but clinically significant. Open conversation, ideally supported by educational resources that partners can access, makes a meaningful difference.
Identity and Self-Perception
For women whose sense of identity has been tied to productivity, competitiveness, or a particular kind of mental sharpness, brain fog can feel like a profound betrayal. The woman who prided herself on never forgetting a face or losing track of a conversation finds herself, suddenly, doing both. This is not character change, it is a symptom. Recognising the difference is the first step toward compassion for yourself.
Workplace Challenges
Research increasingly shows that menopausal symptoms significantly affect workplace performance and confidence, and that women are often reluctant to disclose the cause for fear of stigma or professional disadvantage. Menopause workplace policies are emerging in progressive organisations, but systemic change is slow. Individually, many women find relief in practical adjustments — environmental (a desk fan, a cooler workspace), schedule-related (protecting high-focus work for optimal energy windows), or conversational (selective disclosure to trusted managers or HR).
Menopause is not the end of a woman's productive, creative, passionate life. It is a transition — demanding, yes, but also an opportunity for profound recalibration.
14. The Future of Menopause Care
Personalised Hormone Medicine
The future of menopause treatment is personalised. Advances in genetic testing, biomarker analysis, and hormone profiling are beginning to enable more precisely tailored treatment decisions, moving away from population-level generalisation and toward individual risk-benefit calculation. This shift has the potential to make hormone therapy both safer and more effective for the women who need it most.
Telehealth and Accessibility
Menopause telehealth platforms are rapidly expanding access to qualified menopause specialists, particularly for women in regions or demographics where specialist care has historically been inaccessible. The ability to consult a menopause-trained clinician from home, have prescriptions delivered, and monitor symptoms digitally has already changed the experience of menopause care for many women.
AI-Assisted Symptom Tracking
AI-powered health applications are increasingly capable of identifying patterns in symptom diaries, correlating symptoms with cycle data and lifestyle factors, and surfacing insights that support clinical decision-making. While these tools are not replacements for clinical care, they represent meaningful additions to the informed patient's toolkit.
Better Research
The WHI study's limitations highlighted the need for more rigorous, representative, and nuanced research on women's hormonal health. That research is underway. Ongoing studies are examining the long-term effects of different HRT types on cognitive health, cardiovascular outcomes, and cancer risk in more granular ways. The next decade is likely to yield considerably more detailed guidance.
Cultural Shift
Perhaps most importantly, the cultural conversation around menopause is changing. Women are speaking more openly about their experiences. The workforce is demanding accommodation. Media portrayals are, slowly, becoming more accurate and less dismissive. The generation of women currently navigating perimenopause is the most educated, most connected, and most vocal in history. They are driving change.
15. Frequently Asked Questions
Can estrogen therapy improve brain fog?
For many women, yes, particularly when therapy is initiated relatively early in the menopausal transition and when brain fog is linked to hormonal disruption of cognitive pathways. Evidence is promising but not definitive for all women; the response is individual. Cognitive improvements are often reported alongside improvements in sleep and mood, suggesting a compounding benefit.
At what age should I start thinking about hormone therapy?
There is no universal starting age. If you are experiencing significant perimenopausal symptoms, even in your early-to-mid 40s, a conversation with your doctor about your options is appropriate. The timing hypothesis suggests that for eligible women, earlier initiation relative to menopause onset may offer additional benefits.
How long can I stay on HRT?
Duration is individualised. Many professional societies no longer recommend arbitrary time limits (such as 'no more than 5 years'). Instead, they advocate for regular review, typically annually, to reassess whether benefits continue to outweigh risks for the individual. Some women continue therapy for many years with appropriate monitoring.
Are there non-hormonal medications for menopause symptoms?
Yes. Several non-hormonal medications are used for menopause symptoms. SSRIs and SNRIs (antidepressants) are used for vasomotor symptoms and mood. Gabapentin and pregabalin have evidence for hot flashes and sleep. Fezolinetant, a neurokinin receptor antagonist, is a newer non-hormonal option specifically for hot flashes approved in several countries. Ospemifene is used for genitourinary symptoms. Discuss options with your doctor.
What is the difference between bioidentical and conventional HRT?
'Bioidentical' means the hormone is chemically identical to what the human body produces. Many conventionally prescribed HRT products are bioidentical, including estradiol patches and micronised progesterone. Compounded bioidentical hormones from specialist pharmacies are customised but have less standardised evidence. Speak with your doctor about what this distinction means for your specific prescription.
Does menopause cause permanent memory loss?
Current evidence suggests that cognitive changes during menopause are predominantly transitional, most pronounced during perimenopause and the years immediately following. For the majority of women, cognitive function stabilises post-menopause. Sustained, severe cognitive decline should always be evaluated by a doctor to rule out other causes.
16. Conclusion — You Deserve Clarity, Not Confusion
Menopause is one of the most significant biological transitions a woman will experience, and for too long, it has been managed with silence, dismissal, and insufficient information. That is changing.
Estrogen therapy is not perfect. It is not a miracle. It carries real risks that must be assessed individually and carefully. But for millions of women who are appropriate candidates, it offers real, meaningful, evidence-supported relief, from the brain fog that clouds your thinking, the heat surges that disrupt your sleep, the mood shifts that strain your relationships, and the bone loss that accumulates invisibly over time.
What you feel is real. What you are experiencing has biological explanations and, in many cases, effective treatments. You are not imagining it, you are not overreacting, and you do not have to manage it alone.
Find a clinician who takes your symptoms seriously. Bring your questions. Track your symptoms. And trust yourself — you know your body better than anyone.
The science is evolving. The conversation is finally beginning. And the most important step is the one you take today: asking for the information, the care, and the support you deserve.
Suggested Internal Links
| Suggested Article Title | Suggested URL Slug |
|---|---|
| Understanding Perimenopause: A Complete Timeline | /perimenopause-timeline-guide |
| Menopause and Anxiety: What's Really Happening | /menopause-anxiety-hormones |
| Sleep During Menopause: Strategies That Actually Work | /menopause-sleep-guide |
| Non-Hormonal Menopause Treatments: A Complete Overview | /non-hormonal-menopause-options |
| How to Find a Menopause Specialist Near You | /finding-menopause-specialist |
| Bone Health After 40: Everything You Need to Know | /bone-health-menopause |
| The Mediterranean Diet and Menopause | /mediterranean-diet-menopause |
| Strength Training for Menopausal Women | /strength-training-menopause |
Medical Disclaimer
This article is intended for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any decisions about hormone therapy, supplements, or changes to your health management plan. Individual circumstances vary significantly, and what is appropriate for one person may not be appropriate for another. The author and publisher accept no liability for decisions made based on this content.